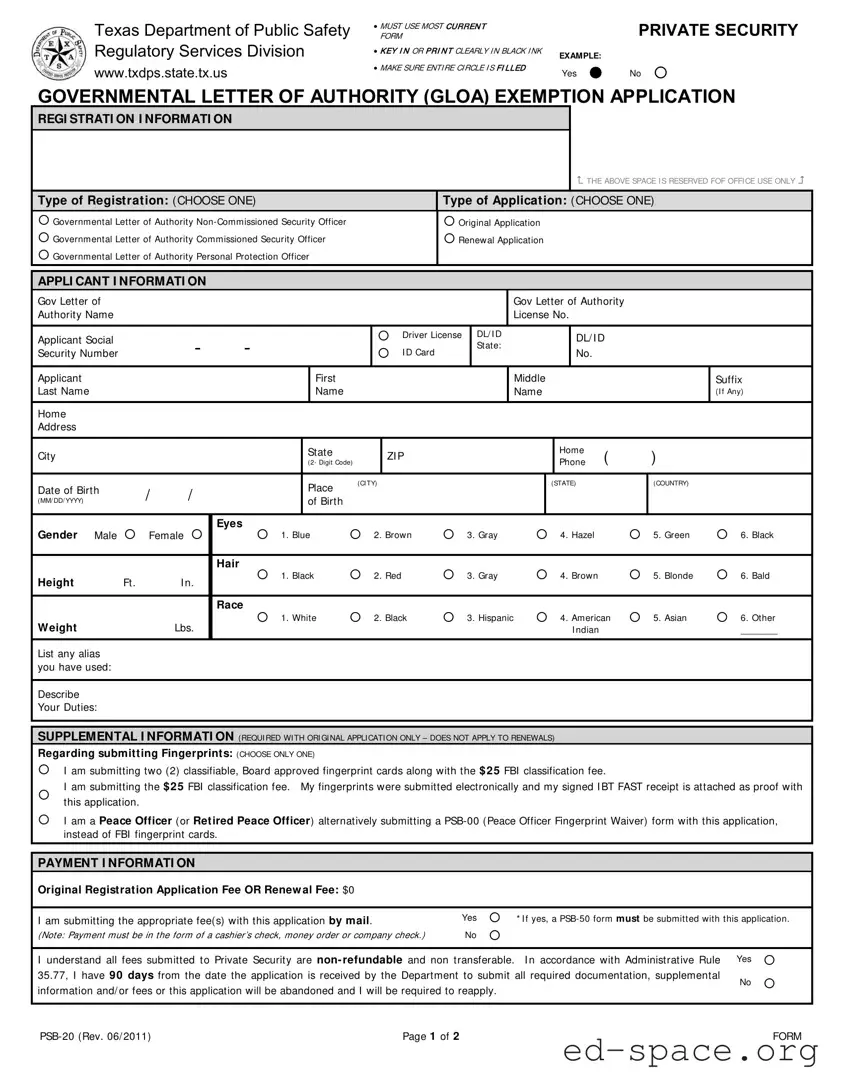
The Texas PSB 20 form is an essential document for individuals seeking registration as security officers within the state. This form is specifically designed for applicants under the Governmental Letter of Authority (GLOA) exemption, allowing them to apply for various types of security roles, including non-commissioned and commissioned security officers, as well as personal protection officers. It requires applicants to provide personal information such as their name, address, date of birth, and social security number, along with details about their employment and responsibilities. Additionally, the form includes sections that address background checks, requiring applicants to disclose any criminal history, military service, and mental health evaluations. Payment information is also outlined, emphasizing that fees are non-refundable and non-transferable. Completing this form accurately is crucial, as any discrepancies or omissions could lead to delays or denials in the application process. It is important to use the most current version of the form and to fill it out clearly, ensuring all required fields are completed to facilitate a smooth review by the Texas Department of Public Safety.
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The Texas PSB 20 form is used for applying for a Governmental Letter of Authority exemption for security officer registration. |
| Governing Law | This form is governed by the Texas Occupations Code §1702, which regulates private security services in the state. |
| Eligibility Requirements | Applicants must meet specific eligibility criteria, including background checks and potential disqualifying offenses. |
| Application Types | Applicants can choose between original or renewal applications for various types of security officer registrations. |
| Payment Information | Fees are non-refundable and must be submitted via cashier’s check, money order, or company check. |
| Supplemental Information | Original applications require additional documentation, including fingerprint submissions or waivers for certain applicants. |
| Background Checks | All applicants must disclose any felony or misdemeanor convictions, pending charges, and certain mental health issues. |
| Signature Requirement | Both the applicant and the employer's representative must sign the form to validate the application. |
| Submission Method | The completed form and any attachments should be mailed to the Texas Department of Public Safety. |
After gathering all necessary information, you can begin filling out the Texas PSB 20 form. Follow these steps carefully to ensure that your application is complete and accurate.
What is the Texas PSB 20 form?
The Texas PSB 20 form is an application used for individuals seeking registration as a non-commissioned or commissioned security officer or personal protection officer in Texas. It is a requirement set by the Texas Department of Public Safety for those who work in the private security industry.
Who needs to fill out the PSB 20 form?
Anyone applying for a registration as a non-commissioned or commissioned security officer or personal protection officer in Texas must complete the PSB 20 form. This includes individuals working under a Governmental Letter of Authority.
What information is required on the PSB 20 form?
The form requires personal information such as your name, address, date of birth, and social security number. It also asks about your background, including any criminal history, military discharge status, and whether you are required to register as a sex offender.
How do I submit fingerprints with the PSB 20 form?
You have a few options for submitting fingerprints. You can provide two classifiable fingerprint cards along with a $25 FBI classification fee, or you can submit electronically and attach the signed receipt. If you are a peace officer, you may submit a PSB-00 form instead.
What is the application fee for the PSB 20 form?
There is no application fee for the original registration or renewal when submitting the PSB 20 form. However, if you choose to submit payment, it must be in the form of a cashier’s check, money order, or company check.
What happens if I do not submit all required documents?
If you do not submit all required documentation within 90 days of your application being received, your application will be abandoned. You will then need to reapply to receive your registration.
Can I apply for a renewal using the PSB 20 form?
Yes, the PSB 20 form can be used for both original applications and renewal applications. Make sure to select the appropriate option when filling out the form.
What if I have a criminal history?
If you have a criminal history, you must disclose this on the form. Depending on the nature of the offenses and how long ago they occurred, this may affect your eligibility for registration.
Where do I send the completed PSB 20 form?
You can mail the completed PSB 20 form and any attachments to the Texas Department of Public Safety, Private Security, MSC 02 42, PO Box 15999, Austin, TX 78761-5999.
Is the PSB 20 form available online?
Yes, you can find the most current version of the PSB 20 form on the Texas Department of Public Safety's website. Always ensure you are using the latest version to avoid any issues with your application.
Using an outdated form: Applicants must ensure they are using the most current version of the Texas PSB 20 form. Using an outdated form can lead to delays or rejections of the application.
Illegible handwriting: It is crucial to fill out the form clearly, either by typing or printing in black ink. Illegible handwriting can cause misunderstandings and may result in the application being deemed incomplete.
Incomplete circles: Applicants must ensure that the entire circle is filled in for responses. Leaving any circles unmarked or partially filled can lead to confusion and potential denial of the application.
Failure to provide required documentation: Some sections of the form require additional documentation, such as proof of fingerprint submission or military discharge papers. Not including these documents can result in the application being rejected.
The Texas PSB 20 form is a critical document for individuals seeking registration as security personnel in Texas. Along with this form, several other documents are commonly used to facilitate the registration process. Each of these documents serves a specific purpose and is essential for ensuring compliance with state regulations.
In summary, the Texas PSB 20 form is typically accompanied by several other important documents that play a vital role in the registration process for security personnel. Each document contributes to verifying the applicant's qualifications and ensuring compliance with state regulations.
The Texas PSB 20 form is essential for individuals seeking to register as security personnel. It shares similarities with several other important documents in the realm of professional licensing and registration. Here are four such documents:
When filling out the Texas PSB 20 form, attention to detail is crucial. Here are some important dos and don'ts to keep in mind:
By following these guidelines, applicants can improve their chances of a smooth application process. Careful attention to the details ensures that all necessary information is provided accurately and completely.
Understanding the Texas PSB 20 form can be challenging, especially with the various misconceptions that exist. Here are seven common misunderstandings clarified to help applicants navigate the process more effectively.
This form is applicable to various types of applicants, including non-commissioned security officers and personal protection officers. It is essential to select the correct type of registration when filling out the form.
Applicants must use the most current version of the PSB 20 form. Using an outdated form may lead to delays or rejection of the application.
Fingerprint submission is required for original applications, but not for renewals. Ensure you choose the correct option regarding fingerprints when completing the form.
Payment is a mandatory part of the application process. Applicants must submit the appropriate fee, which is non-refundable and non-transferable.
All applicants must disclose any criminal history, including pending charges. Failure to report this information may result in denial or revocation of the license.
The application process can take time. Applicants have 90 days to submit all required documentation, or their application may be abandoned, necessitating a new submission.
It is crucial to fill out the PSB 20 form using black ink only. This ensures that the information is clear and legible for processing.
Use the Most Current Form: Ensure that you are filling out the latest version of the Texas PSB 20 form. Using outdated forms may lead to delays or rejections.
Clear and Legible Information: Fill in all information clearly and in black ink. This helps prevent misunderstandings and ensures that your application is processed smoothly.
Complete All Required Sections: Make sure to fill out every section of the form, including personal details, background information, and employment details. Incomplete forms can result in delays.
Governmental Letter of Authority: If you are applying under a Governmental Letter of Authority, select the appropriate option. This is crucial for the processing of your application.
Fingerprint Submission: Choose the correct method for submitting fingerprints. You can either submit fingerprint cards or provide proof of electronic submission. Ensure you follow the instructions carefully.
Payment Information: If applicable, include the correct payment with your application. Remember that payments must be in the form of a cashier's check, money order, or company check.
Background Information: Answer all background questions truthfully. Failing to disclose relevant information may lead to denial or revocation of your application.
Employer Certification: Your employer must complete and sign the employer section of the form. This confirms your employment and the necessity of your registration.
Submit in a Timely Manner: Be aware of the 90-day deadline for submitting all required documentation and fees. Failure to do so may result in your application being abandoned.