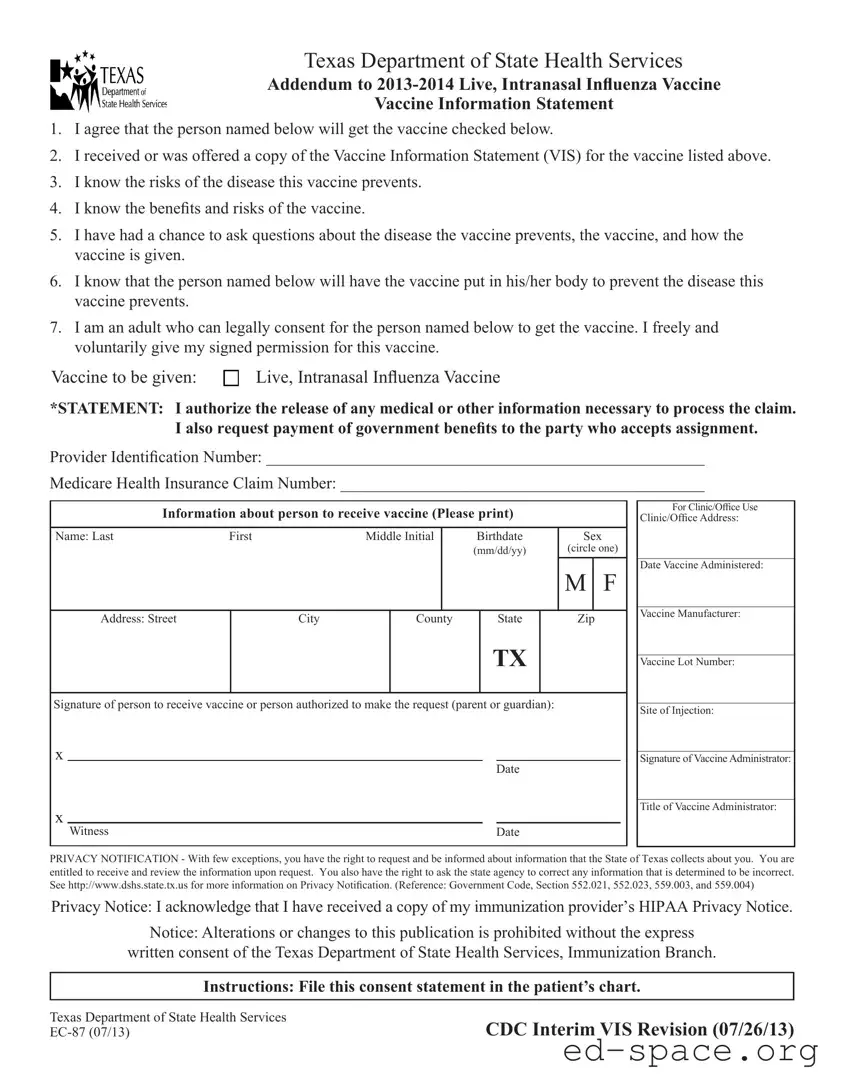
The Texas EC 87 form is an essential document used in the administration of the Live, Intranasal Influenza Vaccine. This form serves multiple purposes, ensuring that individuals receiving the vaccine are fully informed and consenting to the procedure. It includes a series of statements that confirm the recipient understands the risks associated with both the influenza disease and the vaccine itself. By signing the form, the adult providing consent acknowledges that they have received the Vaccine Information Statement and have had the opportunity to ask questions regarding the vaccine and its administration. The form also collects necessary personal information about the individual receiving the vaccine, including their name, birthdate, and address, as well as details related to the vaccination, such as the vaccine manufacturer and lot number. Additionally, it includes a privacy notification, outlining the rights of individuals concerning their personal information collected by the state. This comprehensive approach not only facilitates the vaccination process but also emphasizes the importance of informed consent and privacy in healthcare.
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Texas EC 87 form serves as a consent document for individuals receiving the Live, Intranasal Influenza Vaccine. It ensures that the recipient or their guardian understands the vaccine's risks and benefits. |
| Governing Laws | This form is governed by Texas state laws, specifically the Government Code, Sections 552.021, 552.023, 559.003, and 559.004, which relate to privacy rights and information access. |
| Privacy Notification | The form includes a privacy notification, informing individuals of their rights to access and correct information collected by the State of Texas regarding their immunization. |
| Signature Requirement | A signature is required from the individual receiving the vaccine or an authorized guardian, confirming their voluntary consent for the vaccination. |
To fill out the Texas EC 87 form, gather the necessary information beforehand. This includes the recipient's personal details and the vaccine information. Follow the steps below to complete the form accurately.
What is the Texas EC 87 form?
The Texas EC 87 form is a consent document used for administering the Live, Intranasal Influenza Vaccine. It ensures that individuals or their guardians are informed about the vaccine, its benefits, and the potential risks associated with it. By signing the form, the adult giving consent acknowledges that they understand the information provided and agree to the vaccination for the person named on the form.
Who can sign the Texas EC 87 form?
Only an adult who is legally authorized to provide consent can sign the Texas EC 87 form. This typically includes parents or legal guardians of minors. The form requires the signature of the person receiving the vaccine or the authorized adult, confirming their understanding of the vaccine's purpose and their willingness to proceed with the vaccination.
What information is required on the Texas EC 87 form?
The form requires several key pieces of information. This includes the name, birthdate, and sex of the individual receiving the vaccine, as well as their address. Additionally, the form asks for the provider identification number and Medicare Health Insurance Claim Number if applicable. It is important that this information is accurate to ensure proper documentation and follow-up.
What should I do if I have questions about the vaccine?
If you have questions about the Live, Intranasal Influenza Vaccine, it is important to ask them before signing the Texas EC 87 form. The form states that individuals have the opportunity to ask questions regarding the disease the vaccine prevents, the vaccine itself, and the administration process. Don’t hesitate to reach out to healthcare providers for clarification or additional information.
What happens to the information provided on the Texas EC 87 form?
The information on the Texas EC 87 form is used to document consent for the vaccination and to process any claims related to the vaccine. The Texas Department of State Health Services has strict privacy regulations in place. Individuals have the right to request access to their information and can ask for corrections if they believe any information is incorrect. This ensures transparency and protects personal data.
Can I alter the Texas EC 87 form?
No, alterations or changes to the Texas EC 87 form are prohibited without express written consent from the Texas Department of State Health Services. It is crucial to use the form as it is provided to ensure compliance with state regulations and to maintain the integrity of the vaccination process.
Incomplete Personal Information: Failing to provide all required details such as the full name, birthdate, and address of the individual receiving the vaccine can lead to delays or issues in processing.
Incorrect Vaccine Information: Not specifying the correct vaccine type or failing to check the appropriate box can result in administering the wrong vaccine.
Missing Signatures: Omitting the necessary signatures from the person receiving the vaccine or their authorized guardian can invalidate the consent.
Failure to Read the Vaccine Information Statement: Not reviewing the Vaccine Information Statement (VIS) before signing can lead to a lack of understanding about the vaccine's benefits and risks.
Ignoring the Privacy Notification: Overlooking the privacy notification and not acknowledging receipt of the HIPAA Privacy Notice can create legal complications regarding personal health information.
Incorrect Dates: Writing the wrong date for either the signature or the vaccine administration can cause confusion and complicate record-keeping.
Inaccurate Provider Information: Providing incorrect or incomplete information about the healthcare provider administering the vaccine can hinder the claims process.
Failing to Ask Questions: Not taking the opportunity to ask questions about the vaccine can lead to misunderstandings about its purpose and administration.
Assuming Consent: Assuming that a verbal consent is sufficient instead of providing a written signature can lead to complications and potential liability issues.
Not Keeping a Copy: Failing to keep a copy of the completed form for personal records can create challenges in case of future medical inquiries or claims.
The Texas EC 87 form is often used in conjunction with several other documents that facilitate the administration of vaccines and the management of related information. Below is a list of these forms and documents, each serving a specific purpose.
These documents work together to ensure a smooth vaccination process, protect patient rights, and maintain accurate health records. Familiarity with these forms can help individuals navigate the vaccination process more effectively.
The Texas EC 87 form serves as a consent document for the administration of the live, intranasal influenza vaccine. Several other documents share similarities with this form, particularly in their purpose of obtaining consent, providing information, and ensuring that individuals understand the implications of medical procedures. Below are six documents that are comparable to the Texas EC 87 form:
When filling out the Texas EC 87 form, it is essential to follow certain guidelines to ensure accuracy and compliance. Below is a list of things to do and avoid during this process.
Understanding the Texas EC 87 form is essential for anyone involved in the vaccination process. However, several misconceptions can lead to confusion. Below are some common misunderstandings:
Being informed about these misconceptions can help individuals navigate the vaccination process with greater confidence and clarity.
When it comes to filling out the Texas EC 87 form, understanding its purpose and the information it requires is crucial. Here are some key takeaways to keep in mind:
Understanding these points can help streamline the process of vaccination and ensure that all necessary consent and information are properly documented.