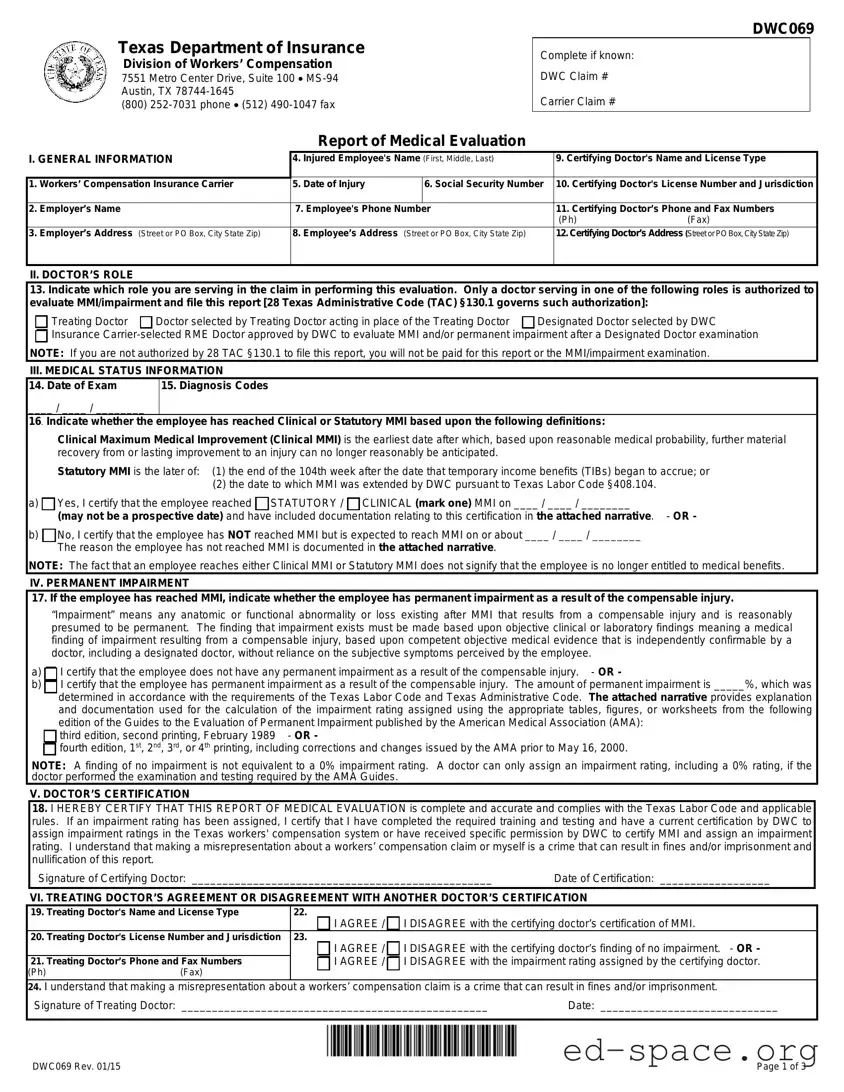
The Texas DWC069 form, also known as the Report of Medical Evaluation, plays a crucial role in the workers' compensation process within the state. This form is designed to document the medical evaluation of an injured employee, providing essential information about their condition and recovery status. It requires details such as the injured employee's name, social security number, and the specifics of their injury, including the date it occurred. The form is filled out by a certifying doctor, who must be authorized to assess Maximum Medical Improvement (MMI) and any permanent impairment resulting from the injury. The doctor’s role is clearly defined, with options for different types of evaluators, including treating doctors and designated doctors. The evaluation must include the doctor’s certification regarding whether the employee has reached MMI and, if applicable, the percentage of permanent impairment. The form also emphasizes the importance of accurate and honest reporting, as misrepresentation can lead to serious consequences. Once completed, the DWC069 must be filed with multiple parties, including the insurance carrier and the injured employee, ensuring transparency and proper communication throughout the claims process.
| Fact Name | Details |
|---|---|
| Governing Law | The DWC069 form is governed by the Texas Labor Code §408.104 and 28 Texas Administrative Code §130.1. |
| Purpose | This form is used to report medical evaluations related to workers' compensation claims in Texas. |
| Filing Deadline | The form must be filed no later than the seventh working day after the examination date or after receiving necessary medical information. |
| Authorized Doctors | Only certain doctors, such as treating doctors or designated doctors, are authorized to complete and submit the DWC069 form. |
| MMI Certification | Doctors must certify whether the injured employee has reached Maximum Medical Improvement (MMI) based on specific criteria. |
| Dispute Process | If an injured employee disagrees with the MMI certification, they can dispute it within 90 days by contacting their local DWC office. |
Completing the Texas DWC069 form is a straightforward process, but it requires careful attention to detail. This form is essential for reporting medical evaluations related to workers' compensation claims. Once you have filled out the form correctly, you will need to submit it to the appropriate parties, including the insurance carrier and the Division of Workers’ Compensation.
After completing the form, ensure that you keep a copy for your records. Then, submit the DWC069 form and any necessary documentation to the insurance carrier, the treating doctor, the Division of Workers’ Compensation, and the injured employee. This submission can usually be done via fax or electronic transmission. It’s important to follow these steps carefully to ensure compliance with Texas workers' compensation regulations.
What is the Texas DWC069 form?
The Texas DWC069 form, officially known as the Report of Medical Evaluation, is a document used in the Texas workers' compensation system. It is primarily utilized by medical professionals to report on an injured employee's Maximum Medical Improvement (MMI) status and any permanent impairment resulting from a workplace injury. This form must be completed by authorized doctors who are involved in the employee's care.
Who is authorized to complete the DWC069 form?
Only specific medical professionals can complete the DWC069 form. These include the treating doctor, a doctor selected by the treating doctor, a designated doctor appointed by the Texas Department of Insurance, and an insurance carrier-selected Required Medical Examination (RME) doctor, provided they have received prior approval from the Division of Workers’ Compensation (DWC).
When must the DWC069 form be filed?
The DWC069 form must be filed no later than the seventh working day after the date of the examination or after receiving all necessary medical information to certify MMI. This requirement applies only if the employee has reached MMI. If the employee has not reached MMI, only a designated doctor is required to file the form.
Where should the DWC069 form be submitted?
The completed DWC069 form should be submitted to several parties: the insurance carrier, the treating doctor (if applicable), the DWC, the injured employee, and the employee’s representative if one exists. The submission can be made via fax or electronic transmission, unless other arrangements have been made.
What happens if I disagree with my doctor’s MMI certification?
If an injured employee disagrees with the doctor’s certification of MMI or the assigned permanent impairment rating, they have the right to dispute it. This can be done by contacting the local DWC field office or calling the DWC directly to request a designated doctor or a Benefit Review Conference (BRC). It’s important to file the dispute within 90 days of receiving the written notice to ensure it is considered.
What documentation must a doctor maintain when filing the DWC069 form?
Doctors must keep the original copy of the DWC069 form along with any narratives and documentation related to the examination. This includes the date of the examination, the date medical records necessary for certification were received, and the details of how the reports were transmitted to the relevant parties.
What is the difference between Clinical MMI and Statutory MMI?
Clinical MMI refers to the earliest date after which further recovery from an injury is not expected based on reasonable medical probability. Statutory MMI, on the other hand, is defined as either the end of the 104th week after temporary income benefits began or the date extended by the DWC. Understanding these distinctions is crucial for both doctors and injured employees.
Where can I find additional information about the DWC069 form?
For more detailed information regarding the DWC069 form and its requirements, individuals can refer to the Texas Department of Insurance website. The complete text of the relevant rules can be found under 28 Texas Administrative Code §130.1 through §130.4 and §130.6. For any further questions, the DWC can be contacted directly at 1-800-372-7713, Option #3.
Incomplete Information: Failing to fill out all required fields can lead to delays. Ensure that every section is completed, including the employee's name, date of injury, and social security number.
Incorrect Dates: Entering prospective dates for MMI certification is a common mistake. The date of MMI must reflect an actual date, not a future date.
Missing Documentation: Not attaching necessary documentation to support the MMI certification can invalidate the report. Include all relevant narratives and medical records.
Unauthorized Signatures: Having someone other than the certifying doctor sign the form is a serious error. Only the doctor who performed the evaluation should sign the report.
Incorrect Role Selection: Misidentifying the role of the doctor in the claim can lead to complications. Ensure the correct role is selected from the options provided on the form.
The Texas DWC069 form, known as the Report of Medical Evaluation, is an essential document in the workers' compensation process. It is primarily used to certify an injured employee's Maximum Medical Improvement (MMI) and any permanent impairment resulting from their injury. Alongside this form, several other documents are commonly utilized to ensure a comprehensive understanding of the case and to facilitate the claims process. Below is a list of these documents, each with a brief description.
Understanding these forms and their purposes can significantly aid in navigating the complexities of the Texas workers' compensation system. Each document plays a crucial role in ensuring that injured employees receive the appropriate medical evaluations and benefits they are entitled to, fostering a smoother claims process for all parties involved.
The Texas DWC069 form, known as the Report of Medical Evaluation, shares similarities with several other important documents used in workers' compensation cases. Here are seven documents that are comparable to the DWC069 form, along with a brief explanation of how they relate:
Understanding these forms and their similarities can help both employees and employers navigate the complexities of workers' compensation claims more effectively.
When filling out the Texas DWC069 form, it's important to follow certain guidelines to ensure accuracy and compliance. Here’s a list of things you should and shouldn’t do:
Understanding the Texas DWC069 form is crucial for anyone involved in the workers' compensation process. However, several misconceptions can lead to confusion. Here are six common myths about the DWC069 form, along with clarifications to help clear the air.
This is not true. While treating doctors often file the form, other qualified doctors, such as designated doctors or those selected by the insurance carrier, can also submit it if they are authorized to evaluate MMI and impairment.
This is a misconception. The form is required for both employees who have reached MMI and those who have not. If an employee has not reached MMI, the designated doctor must still file the form to document their status.
This is incorrect. A doctor can only assign any impairment rating, including a 0%, if they have performed the necessary examination and testing as outlined by the AMA Guides. Simply stating there is no impairment is not enough.
This is misleading. Reaching MMI does not mean that an employee loses their right to medical benefits. They may still be eligible for ongoing medical care as needed.
This is false. The form must be filed no later than the seventh working day after the examination or after all necessary medical information has been received. Timeliness is key in this process.
This is incorrect. Employees have the right to dispute the certification of MMI or the impairment rating within 90 days of receiving notice. This ensures that employees can challenge any discrepancies they believe exist.
By addressing these misconceptions, individuals can navigate the workers' compensation process with greater confidence and clarity. Understanding the nuances of the DWC069 form is essential for both employees and medical professionals involved in these claims.
The Texas DWC069 form is a crucial document in the workers' compensation process. Here are key takeaways for its completion and use:
Understanding these points can help ensure that the DWC069 form is filled out correctly and serves its intended purpose in the workers' compensation process.