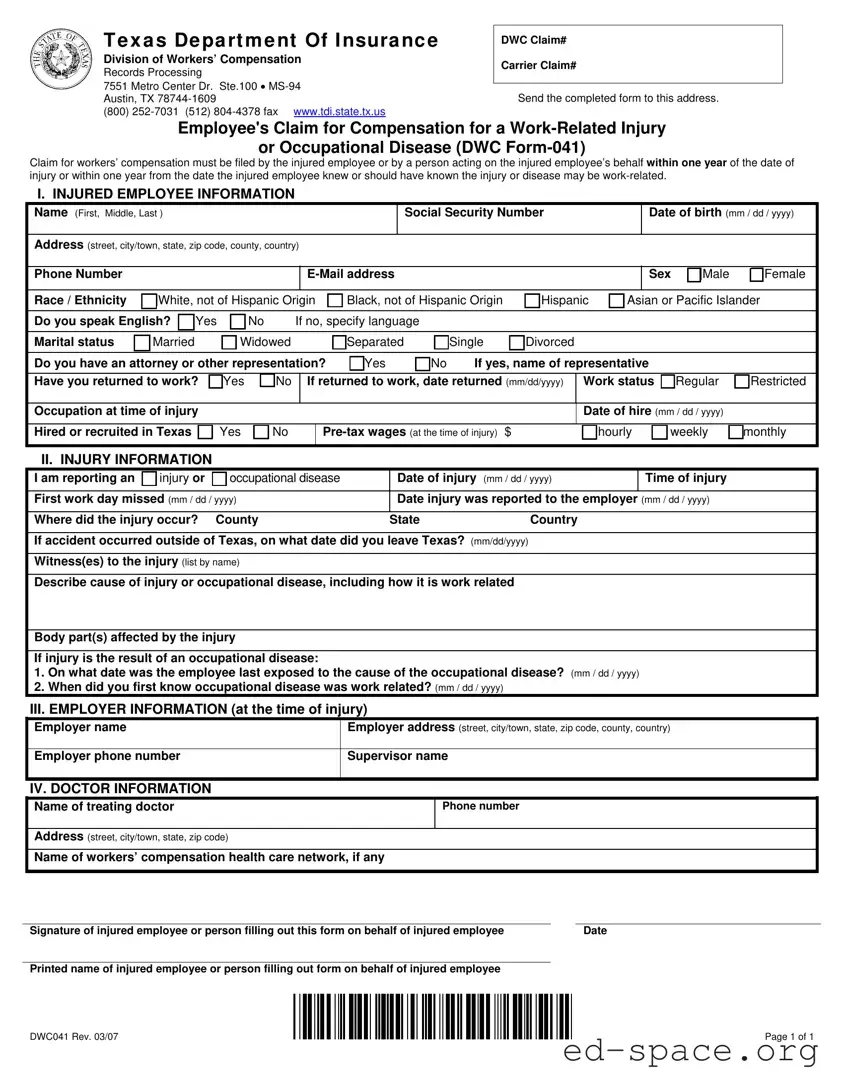
The Texas DWC041 form is a crucial document for employees seeking workers' compensation benefits after a work-related injury or occupational disease. This form must be submitted by the injured employee or a designated representative within one year of the injury or when the employee becomes aware of a work-related condition. Key sections of the DWC041 include personal information about the injured employee, details regarding the injury itself, and information about the employer at the time of the incident. Completing the form accurately is essential, as it initiates the claims process with the Texas Division of Workers’ Compensation. Upon receipt, the Division will assign a claim number and provide important information about the workers' compensation system. Additionally, the form requires specifics about the treating doctor and any relevant health care networks. Adhering to the instructions and providing complete information can significantly impact the outcome of the claim.
| Fact Name | Details |
|---|---|
| Filing Deadline | A claim must be filed within one year of the injury date or from when the employee knew or should have known the injury was work-related. |
| Governing Law | The DWC Form-041 is governed by Texas Labor Code § 408.001. |
| Claim Creation | Upon receipt of the completed form, the Division of Workers' Compensation will create a claim and assign a DWC claim number. |
| Contact Information | For questions, individuals can call the Texas Department of Insurance at 1-800-252-7031. |
Once the Texas DWC041 form is completed, it should be sent to the address provided at the top of the form. This initiates the process for filing a claim for workers' compensation benefits. The Division of Workers' Compensation will then create a claim number and send you further information regarding your claim.
Once completed, ensure all sections are filled accurately before mailing the form to the specified address. This will help facilitate the processing of your claim efficiently.
What is the Texas DWC041 form?
The Texas DWC041 form, also known as the Employee's Claim for Compensation for a Work-Related Injury or Occupational Disease, is a document that employees must complete to file a claim for workers' compensation benefits. This form must be submitted either by the injured employee or by someone acting on their behalf within one year of the injury or when the employee became aware that the injury or disease might be work-related.
Who should fill out the DWC041 form?
The form should be filled out by the injured employee themselves or by a representative acting on their behalf. This may include a family member, legal representative, or another individual authorized to assist with the claim process. Accurate and complete information is crucial for the claim to be processed efficiently.
What information is required on the DWC041 form?
The DWC041 form requires detailed information about the injured employee, including their personal details, work status, and specifics about the injury or occupational disease. This includes the date and time of the injury, the location where it occurred, and any witnesses present. Additionally, information about the employer at the time of injury and the treating doctor must also be provided.
What happens after I submit the DWC041 form?
Upon receiving your completed DWC041 form, the Division of Workers’ Compensation will create a claim and assign a DWC claim number. They will send you information regarding workers' compensation in Texas, as well as notify your employer and their insurance carrier about your claim. This process ensures that all parties are informed and can proceed with the necessary steps.
What if I miss the one-year filing deadline?
If you miss the one-year deadline to file your claim, it may still be possible to proceed if you can demonstrate good cause for the delay. Additionally, if your employer or their insurance carrier does not contest your claim, you may still be able to receive benefits. It is advisable to consult with a legal representative to explore your options in such cases.
Can I get help with filling out the DWC041 form?
Yes, assistance is available for completing the DWC041 form. You can contact your local Division Field Office at 1-800-252-7031 for guidance. They can provide answers to any questions you may have about the form or the workers' compensation process in Texas.
What should I do if I need to correct information on my claim?
If you find that any information on your claim is incorrect, you have the right to request a correction. Under Texas Government Code provisions, you can contact the Division’s Open Records section at 512-804-4437 to address inaccuracies in your claim information. Ensuring that your records are correct is essential for a smooth claims process.
Incomplete Information: Failing to fill out all required fields can lead to delays. Ensure that every section is completed, including personal details and injury specifics.
Incorrect Dates: Providing wrong dates, such as the date of injury or the date the injury was reported, can complicate your claim. Double-check all dates for accuracy.
Missing Signatures: Not signing the form can result in rejection. Always ensure that the injured employee or their representative has signed the form before submission.
Omitting Employer Information: Failing to include accurate employer details can hinder the processing of your claim. Verify that the employer's name and address are correct.
Neglecting to Specify Work Status: Not indicating whether you have returned to work and your current work status can lead to confusion. Clearly state your work status at the time of filing.
The Texas DWC041 form is a crucial document for employees seeking compensation for work-related injuries or occupational diseases. Alongside this form, several other documents are commonly used to support the claims process. Understanding these documents can help streamline the filing process and ensure that all necessary information is provided.
Using these documents in conjunction with the Texas DWC041 form can enhance the clarity and effectiveness of a workers' compensation claim. Ensuring that all necessary paperwork is completed accurately and submitted promptly can significantly impact the outcome of the claim process.
The Texas DWC041 form is essential for filing a workers' compensation claim in Texas. Several other documents serve similar purposes in different contexts or jurisdictions. Here are four documents that share similarities with the Texas DWC041 form:
Each of these forms is designed to facilitate the claims process for workers' compensation, ensuring that injured employees receive the necessary support and benefits in a timely manner.
When filling out the Texas DWC041 form, it is essential to approach the process with care and attention to detail. Below are some important dos and don'ts to keep in mind.
By adhering to these guidelines, you can help ensure that your claim for workers' compensation is submitted correctly and efficiently. If you have questions while filling out the form, do not hesitate to contact your local Division Field Office for assistance.
There are several misconceptions about the Texas DWC041 form that can lead to confusion for injured employees. Here are eight common misunderstandings, along with explanations to clarify them.
While it's important to file a claim promptly, the form can be submitted within one year from the date of the injury or when the employee realized the injury was work-related.
In fact, a person acting on behalf of the injured employee can also complete the DWC041 form, making it easier for those who may be unable to do so themselves.
Regardless of the perceived severity of the injury, filing the DWC041 form is essential to ensure that the employee's rights to compensation are protected.
Submitting the form does not guarantee that the claim will be approved. The Division of Workers’ Compensation will review the claim and determine eligibility based on the information provided.
Returning to work does not negate the right to file a claim. Employees can still submit the DWC041 form even if they have resumed their duties.
The DWC041 form requires detailed information about the injury, the employer, and the treating doctor. Completing all sections thoroughly is crucial for a successful claim.
Filing the form after the one-year deadline can result in the loss of the right to compensation. Timeliness is essential in the claims process.
It’s wise to keep a copy of the completed DWC041 form for personal records. This can be helpful for future reference or if any issues arise with the claim.
Filling out the Texas DWC041 form is a crucial step in initiating a workers' compensation claim. Here are some key takeaways to keep in mind:
Being thorough and prompt in your submission can significantly impact the outcome of your workers' compensation claim.