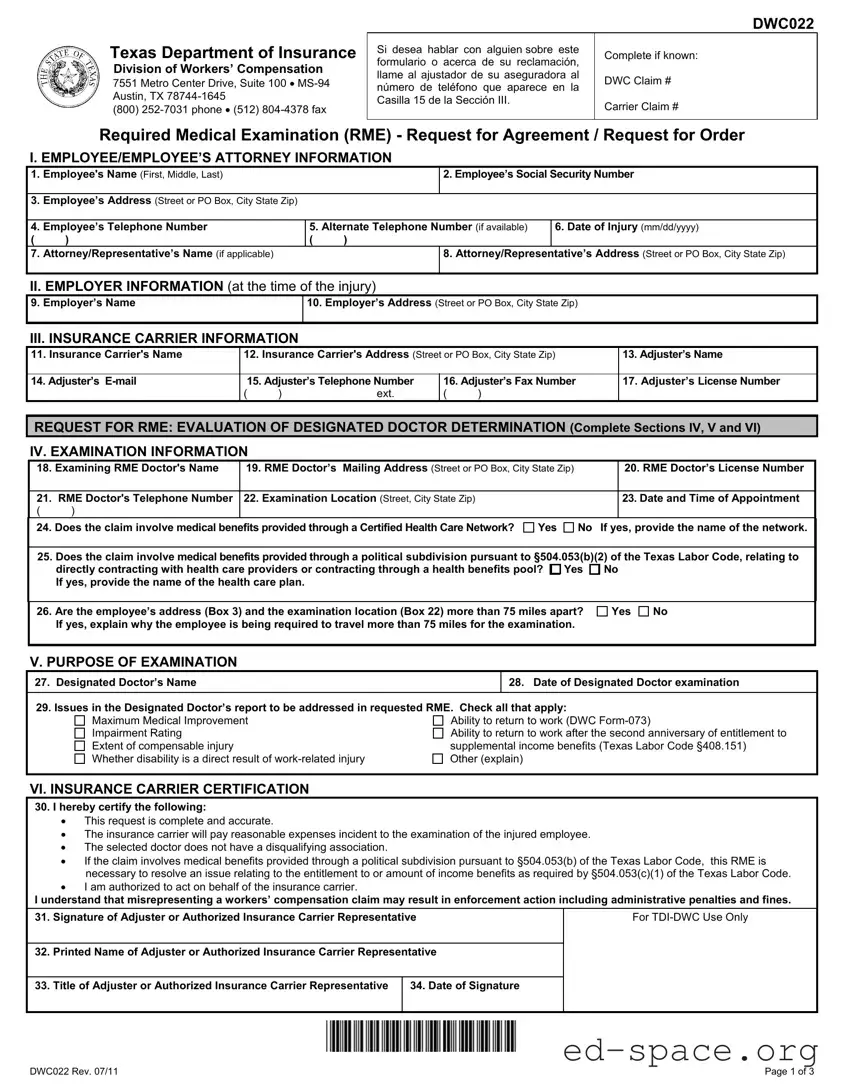
The Texas DWC022 form plays a crucial role in the workers' compensation process, specifically concerning Required Medical Examinations (RMEs). This form is primarily utilized by insurance carriers to request an examination of an injured employee by a doctor of their choice. It serves two main purposes: to evaluate the determination made by a designated doctor and to assess the appropriateness of health care that the employee has received. The form collects essential information about the employee, employer, and insurance carrier, ensuring that all parties are accurately represented. Sections of the form require details such as the employee's name, date of injury, and the specifics of the examination, including the doctor’s information and appointment details. Additionally, the form includes sections for the insurance carrier to certify the accuracy of the request and for the injured employee to indicate their agreement or disagreement with attending the examination. Understanding the DWC022 form is vital for both employees and insurance representatives, as it outlines the necessary steps and obligations involved in the RME process.
| Fact Name | Fact Details |
|---|---|
| Form Purpose | The Texas DWC022 form is used for requesting a Required Medical Examination (RME) related to workers' compensation claims. |
| Governing Law | This form is governed by the Texas Labor Code, particularly §408.004 and §504.053. |
| Employee Information | Section I collects essential details about the employee, including name, Social Security number, and contact information. |
| Employer Details | Section II requires information about the employer at the time of the injury, such as the employer's name and address. |
| Insurance Carrier Info | Section III gathers information about the insurance carrier, including the adjuster's name and contact details. |
| Examination Purpose | Sections IV and V specify the purpose of the examination, which may include evaluating medical improvement or determining the appropriateness of care received. |
| Travel Requirements | If the employee's address and examination location are over 75 miles apart, an explanation must be provided in the form. |
| Certification | The insurance carrier must certify the accuracy of the information provided and ensure compliance with the Texas Labor Code. |
Filling out the Texas DWC022 form is a straightforward process, but it requires attention to detail. This form is essential for requesting a Required Medical Examination (RME) related to workers' compensation claims. Follow these steps to ensure you complete it accurately.
Once the form is filled out, make sure to keep a copy for your records. Submit the completed form to the appropriate parties as directed. This process is crucial for moving forward with any required medical evaluations related to the workers' compensation claim.
What is the Texas DWC022 form used for?
The Texas DWC022 form is used by insurance carriers to request a Required Medical Examination (RME) for an injured employee. There are two main purposes for this form. First, it can be used to evaluate a determination made by a Designated Doctor regarding the employee's medical condition. Second, it can be used to assess whether the health care received by the employee was appropriate. The form must be filled out completely and accurately to ensure the request is processed smoothly.
How often can a Required Medical Examination be performed?
An RME to determine the appropriateness of health care can be performed no more than once every 180 days. However, examinations to evaluate a Designated Doctor’s determination may occur more frequently. If the employee has received Supplemental Income Benefits for eight quarters, the RME regarding their ability to return to work can be conducted no more than once a year.
What happens after the insurance carrier submits the DWC022 form?
Once the Texas Department of Insurance, Division of Workers’ Compensation (TDI-DWC) receives the insurance carrier’s request for an RME, they will review it within 7 days. TDI-DWC will either approve or deny the request. If approved, an order will be issued requiring the employee to attend the examination. If denied, the employee will receive a copy of the denial order, and they will not be required to attend the RME.
Can the RME appointment be rescheduled?
If an employee cannot attend the scheduled RME, they must contact the doctor's office at least 24 hours in advance to reschedule. The new appointment should take place no later than 7 days after the original date. If more time is needed, the employee and the doctor can agree on a different date, but it must be within 30 days of the original appointment.
What should an employee do if they disagree with the RME?
If an employee does not agree to attend the RME, they must complete Section IX of the DWC022 form and return it to the insurance carrier. They have 15 days from the date of the request to respond. If the employee refuses to attend, the insurance carrier may still ask TDI-DWC to issue an order requiring attendance at the examination.
How can employees get information about travel reimbursement for the RME?
Employees can contact the TDI-DWC at (800) 252-7031 for questions about the DWC022 form, accommodations under the Americans with Disabilities Act, or travel reimbursement. To request reimbursement for travel expenses, employees must use the DWC-Form 048, which is available on the TDI website.
Missing Information: Failing to fill out all required fields can lead to delays. Each section must be completed accurately.
Incorrect Dates: Entering the wrong date of injury or appointment can cause confusion. Always double-check these details.
Wrong Social Security Number: Providing an incorrect Social Security number can complicate the claim process. Ensure this number is accurate.
Inaccurate Contact Information: Listing outdated or incorrect addresses and phone numbers can hinder communication. Verify all contact details.
Neglecting to Sign: Forgetting to sign the form can render it invalid. Always ensure that the required signatures are present.
Not Providing Explanations: If the employee's address and examination location are over 75 miles apart, a clear explanation is necessary. Failing to provide this can lead to rejection.
Ignoring Deadlines: Submitting the form after the required deadline can result in complications. Be mindful of all timelines.
Incomplete Certification: The insurance carrier's certification must be complete and accurate. Omitting necessary details can cause issues.
Overlooking Network Claims: If medical benefits are through a certified network, be aware that an RME request may not be appropriate. Understanding this is crucial.
The Texas DWC022 form is a crucial document in the workers' compensation process, particularly for managing Required Medical Examinations (RMEs). However, several other forms and documents often accompany this form to ensure a comprehensive approach to handling claims and examinations. Below is a list of these related documents, each serving a specific purpose in the process.
Each of these forms plays a vital role in the workers' compensation system in Texas. Understanding their purposes can help injured employees navigate the complexities of their claims and ensure they receive the benefits to which they are entitled. Properly completing and submitting these forms can significantly influence the outcome of a claim, making it essential to approach each step with care and attention.
The Texas DWC022 form, which is a request for a Required Medical Examination (RME), shares similarities with several other important documents in the realm of workers' compensation and medical evaluations. Below are five documents that have comparable purposes or functions:
When filling out the Texas DWC022 form, there are several important dos and don’ts to keep in mind. Following these guidelines can help ensure that the process goes smoothly.
This is not true. The DWC022 form can be used for any employee who is involved in a workers' compensation claim, regardless of the severity of their injury. It is meant to facilitate required medical examinations for various situations.
While the form is necessary to request an examination, it does not guarantee approval. The Texas Department of Insurance, Division of Workers' Compensation (TDI-DWC) must review the request and can either approve or deny it.
In fact, employees must respond within 15 days of receiving the request. If they do not respond, the insurance carrier may proceed with further actions, including requesting an order from TDI-DWC.
Ignoring the examination is not an option. If an employee does not agree to attend, the insurance carrier may still seek an order from TDI-DWC requiring attendance. Failure to comply could lead to penalties.
This form can be used for various types of evaluations, including those related to mental health issues that arise from work-related incidents. It addresses the overall appropriateness of care received.
While accuracy is important, minor errors may not invalidate the form. However, all essential information should be completed to avoid delays in processing the request.