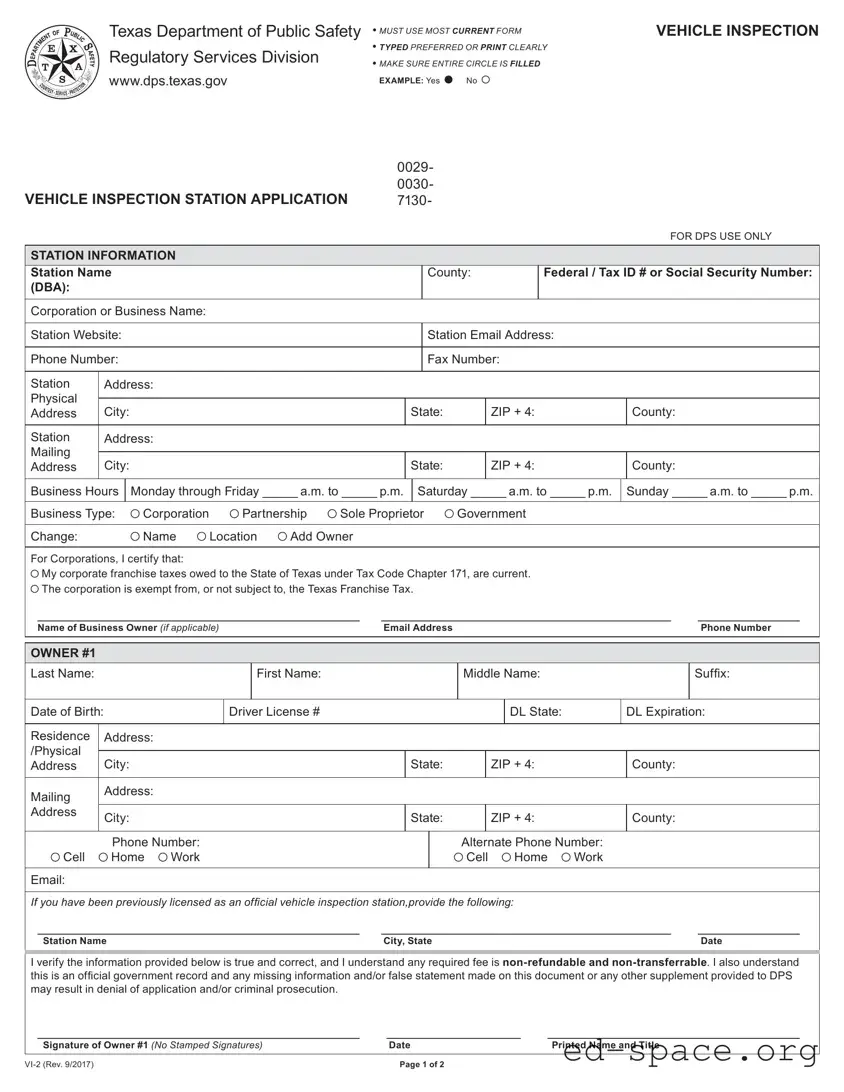
The Texas DPS VI-2 form is essential for individuals and businesses seeking to operate as official vehicle inspection stations in Texas. This form collects vital information about the station, including its name, location, and contact details. Applicants must provide their Federal Tax ID or Social Security number, along with business type, which can be a corporation, partnership, sole proprietorship, or government entity. The form also requires details about the owners of the station, including their names, addresses, and driver’s license information. Additionally, it includes a section for previous inspection station licenses, allowing for a smooth transition for those renewing their applications. Accurate completion of this form is crucial, as any missing or false information may lead to application denial or legal consequences. The form emphasizes the importance of providing truthful data and outlines the non-refundable nature of any fees associated with the application process. Understanding the requirements and ensuring all information is clear and complete will help facilitate a successful application with the Texas Department of Public Safety.

| Fact Name | Details |
|---|---|
| Form Purpose | The Texas DPS VI-2 form is used to apply for a vehicle inspection station license. |
| Submission Requirements | Applicants must fill out the form completely and accurately. Typed submissions are preferred, but clear handwriting is acceptable. |
| Governing Law | This form is governed by the Texas Transportation Code and related regulations. |
| Privacy Notice | Individuals have the right to request information collected about them and to correct any inaccuracies, as stated in Section 559.003 of the Government Code. |
Completing the Texas DPS VI-2 form requires attention to detail and accuracy. After filling out the form, it will be submitted to the Texas Department of Public Safety for processing. Ensure that all required fields are completed and that the information provided is truthful and correct.
What is the Texas DPS VI-2 form?
The Texas DPS VI-2 form is an application for a vehicle inspection station. It is required for businesses that wish to become licensed to conduct vehicle inspections in Texas. The form collects important information about the station, including its name, address, and ownership details. It also includes sections for verifying the owner's information and compliance with state regulations.
Who needs to fill out the VI-2 form?
Anyone who wants to operate a vehicle inspection station in Texas must complete the VI-2 form. This includes individuals and businesses, whether they are corporations, partnerships, or sole proprietors. If you have been previously licensed as an inspection station, you will also need to provide that information on the form.
How should the VI-2 form be completed?
The form should be filled out using the most current version available. It is preferred that you type the information, but if you must write it, please print clearly. Make sure to fill in all required fields completely. Incomplete forms can lead to delays or denial of your application.
What happens if I provide false information on the form?
Providing false information on the VI-2 form can have serious consequences. It may result in the denial of your application, and in some cases, it could lead to criminal prosecution. It is crucial to ensure that all information you provide is accurate and truthful.
Are there any fees associated with submitting the VI-2 form?
Yes, there are fees associated with the application process. These fees are non-refundable and non-transferable. Be prepared to submit payment along with your application. Make sure to check the latest fee schedule on the Texas Department of Public Safety's website for the most accurate information.
Where can I find more information about the VI-2 form?
For more details about the VI-2 form and the vehicle inspection process, you can visit the Texas Department of Public Safety's official website. They provide comprehensive resources and guidelines that can help you understand the requirements and procedures involved in becoming a licensed vehicle inspection station.
Using an outdated form: Always ensure you are using the most current version of the Texas DPS VI-2 form. Using an outdated form may lead to delays or rejection of your application.
Not typing or printing clearly: Fill out the form using a typewriter or print clearly. Illegible handwriting can cause confusion and errors in processing.
Incomplete circles: Make sure to fill in entire circles completely when answering yes or no questions. Incomplete markings may be interpreted as unclear responses.
Missing required information: Double-check that all required fields are filled out completely. Missing information can lead to application denial.
Incorrect business type selection: Ensure that you accurately select the appropriate business type. An incorrect selection can affect your eligibility.
Not providing accurate owner information: Fill in all details for each owner, including full names, dates of birth, and contact information. Inaccurate details may result in complications.
Failing to sign the form: Remember that both owners must sign the application. A missing signature can lead to immediate rejection of your submission.
Ignoring the certification statement: Acknowledge and understand the certification statement regarding the truthfulness of the information provided. Failing to do so can have serious consequences.
Not keeping a copy: Always retain a copy of the completed form for your records. This can be helpful for future reference or in case of disputes.
The Texas DPS VI-2 form is essential for vehicle inspection station applications in Texas. Along with this form, several other documents may be required or helpful in the application process. Below are five common forms and documents often used in conjunction with the VI-2 form.
Having these documents ready can streamline the application process for a vehicle inspection station. It ensures compliance with state regulations and helps avoid any delays in getting the necessary approvals.
The Texas DPS VI-2 form is a vehicle inspection station application. It shares similarities with several other documents used in various regulatory contexts. Below is a list of seven documents that are comparable to the Texas DPS VI-2 form, along with a brief explanation of how they are similar.
When filling out the Texas DPS VI-2 form, attention to detail is crucial. Here are some key do's and don'ts to keep in mind:
By following these guidelines, you can help ensure a smoother application process and avoid common pitfalls associated with the Texas DPS VI-2 form.
Understanding the Texas DPS VI-2 form can be challenging due to some common misconceptions. Here are five of those misconceptions explained:
This form is mandatory for any entity wishing to operate as an official vehicle inspection station in Texas. Without it, you cannot legally conduct vehicle inspections.
Only the owner or authorized representative of the business can complete and sign the VI-2 form. This ensures that the information provided is accurate and legally binding.
You must use the most current version of the VI-2 form. Using an outdated version could lead to delays or rejection of your application.
The Texas Department of Public Safety takes privacy seriously. Personal information collected is protected under state law, and individuals have rights regarding their data.
Providing false information on the VI-2 form can lead to serious consequences, including denial of the application and potential legal action. Accuracy is crucial.
When filling out the Texas DPS VI-2 form, here are some essential points to keep in mind:
By following these guidelines, you can streamline the process of completing the Texas DPS VI-2 form and ensure that your application is processed smoothly.