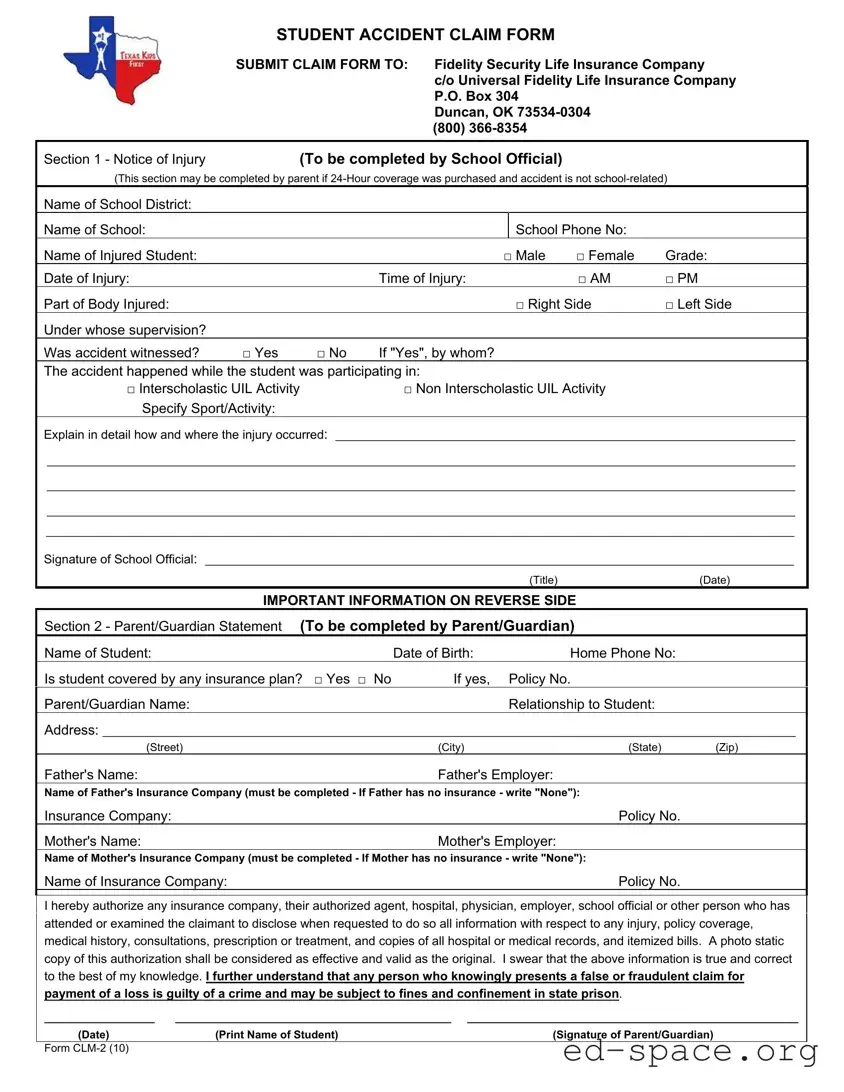
The Texas CLM 2 form serves as a crucial document for parents and guardians navigating the process of filing a student accident claim. Designed to streamline the claims process, this form is divided into two main sections. The first section is completed by a school official and gathers essential information about the injury, including the student’s name, the circumstances surrounding the accident, and the supervision details. It helps establish whether the incident occurred during a school-related activity or not. The second section is filled out by the parent or guardian, requiring personal details about the student, insurance coverage, and an authorization for the release of medical information. This ensures that all parties involved can access necessary records efficiently. Parents should note that the school is not responsible for medical payments, and understanding the claims process is vital. Completing the form accurately and submitting it within the required timeframe can significantly impact the outcome of the claim. Additionally, the Texas Kids First Provider Network offers unique access to medical professionals who are willing to treat injured students without balance billing, further easing the burden on families during challenging times.
| Fact Name | Details |
|---|---|
| Form Purpose | The Texas CLM 2 form is used to file claims for student accidents that occur during school-related activities. |
| Submitting Authority | Claims must be submitted to Fidelity Security Life Insurance Company through Universal Fidelity Life Insurance Company. |
| Completion Requirements | Section 1 is filled out by a school official for school-related accidents, while Section 2 is completed by a parent or guardian. |
| Filing Deadline | The claim form must be submitted within 90 days from the date of the injury. |
| Insurance Coverage | The form requires information about any existing insurance plans covering the injured student. |
| Governing Law | This form is governed by Texas state laws regarding student accident insurance and claims. |
Filling out the Texas Clm 2 form is a straightforward process. This form is essential for filing a claim related to student accidents. Follow the steps carefully to ensure that all necessary information is provided accurately.
Once the form is completed, submit it to the Claims Office at the specified address or electronically. Ensure that all required documents, including itemized bills and any relevant Explanation of Benefits from your primary insurance, are included with your submission. Keep a copy of everything for your records.
What is the Texas CLM 2 form used for?
The Texas CLM 2 form, also known as the Student Accident Claim Form, is utilized to report and process claims for injuries that occur to students during school-related activities. This form is crucial for parents and guardians seeking financial assistance for medical expenses resulting from such injuries. It must be filled out accurately and submitted within 90 days of the incident to ensure proper processing.
Who is responsible for completing the different sections of the form?
The Texas CLM 2 form consists of two main sections. Section 1 is to be completed by a school official for school-related injuries. However, if the injury occurred outside of school activities and 24-Hour coverage was purchased, a parent or guardian may fill out this section. Section 2 must always be completed by the parent or guardian, providing necessary personal and insurance information. This division ensures that all relevant details are captured for a thorough review of the claim.
How should I submit the Texas CLM 2 form?
To submit the Texas CLM 2 form, first, complete both sections as required. The completed form can be sent to the Claims Office at Fidelity Security Life Insurance Company via mail or electronically at [email protected]. It is important to keep a copy of the form for your records and to present a copy to any medical provider involved. Remember, the form must be submitted within 90 days of the injury, regardless of other insurance coverage.
What should I do if I have other insurance?
If you have other insurance coverage for your child, you should first file a claim with that primary insurance provider. After receiving payment or an Explanation of Benefits (EOB) from your primary insurer, submit a copy of the Texas CLM 2 form along with any itemized bills and the EOB to the address provided on the form. This process ensures that you maximize your benefits and that the school’s policy, which is supplemental, is applied correctly.
Incomplete Information: Failing to fill out all required fields can lead to delays. Ensure that every section, including names, dates, and insurance details, is fully completed.
Incorrect Submission: Submitting the form to the wrong address can result in denial of the claim. Always send it to the specified address: Fidelity Security Life Insurance Company, P.O. Box 304, Duncan, OK 73534-0304.
Missing Signatures: Neglecting to sign the form can halt the processing. Both the school official and the parent/guardian must provide their signatures where required.
Failure to Submit on Time: The claim form must be submitted within 90 days of the injury. Missing this deadline can result in automatic denial of the claim.
Not Including Itemized Bills: Submitting only monthly statements instead of itemized bills can lead to complications. Ensure to include original itemized bills that detail the services provided.
The Texas Clm 2 form is a crucial document for filing a student accident claim. However, several other forms and documents often accompany it to ensure a smooth claims process. Below is a list of these related documents, each serving a specific purpose.
These documents work together to facilitate the claims process and ensure that all necessary information is available for review. Properly completing and submitting these forms can help streamline the resolution of the claim.
The Texas Clm 2 form serves as a critical document for filing claims related to student accidents. There are several other forms that share similar purposes or functions. Below are four documents that are comparable to the Texas Clm 2 form:
Understanding these similarities can help individuals navigate the claims process more effectively, ensuring that all necessary information is provided for a successful outcome.
When filling out the Texas Clm 2 form, there are several important dos and don’ts to keep in mind. Following these guidelines can help ensure your claim is processed smoothly.
By following these steps, you can help make the claims process easier and more efficient.
Understanding the Texas Claim 2 form can be challenging. Here are some common misconceptions about this form:
This is not true. The school may have purchased a supplemental policy, but parents are generally responsible for any costs not covered by insurance.
Parents must still submit the claim form even if they have other insurance. The school’s policy is supplemental.
The claim form must be submitted within 90 days of the injury. Delays can result in denial of the claim.
While Section 1 must be completed by a school official, parents can fill out the form if they purchased 24-hour coverage and the injury is not school-related.
The Texas Kids First policy is a limited benefit policy. It may not cover all medical expenses incurred.
It is essential for parents to submit the claim themselves. Do not depend on providers to handle this process.
The TKF Network operates independently and is not connected to Fidelity Security Life Insurance Company.
It is crucial to keep copies of the claim form and itemized bills for your records. This can help in case of any disputes.
Filling out the Texas Clm 2 form can seem overwhelming, but understanding its key components can make the process smoother. Here are some important takeaways:
By following these steps and understanding the form's requirements, you can effectively navigate the claims process. If you have questions, don't hesitate to reach out to your school trainer or the provided contact number.