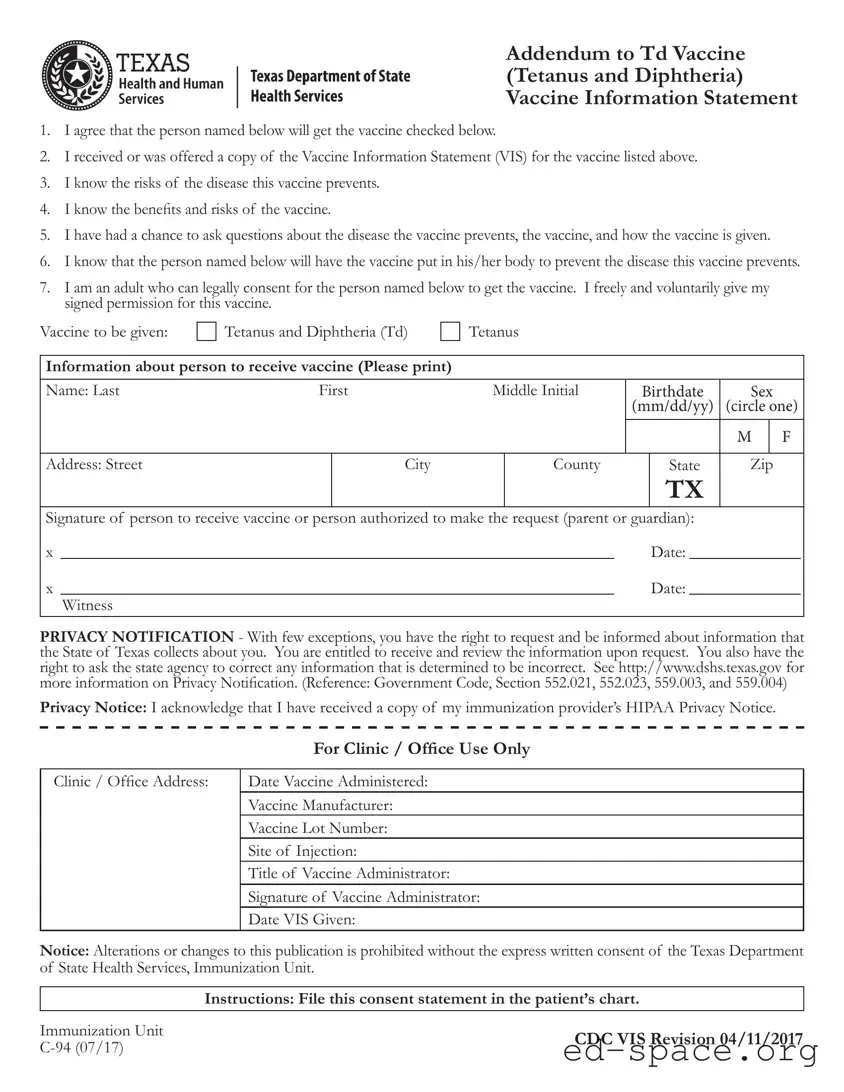
The Texas Addendum to the Tdap Vaccine form serves as a crucial document in the immunization process, ensuring that individuals receive the necessary information and consent for the Tetanus and Diphtheria (Td) vaccine. This form outlines the responsibilities of both the vaccine recipient and the adult providing consent, typically a parent or guardian. It emphasizes the importance of understanding the risks associated with the diseases the vaccine prevents, as well as the benefits and potential risks of the vaccine itself. Individuals signing the form confirm that they have received or been offered a Vaccine Information Statement (VIS) and have had the opportunity to ask questions regarding the vaccine. Additionally, the form requires essential information about the person receiving the vaccine, including their name, birthdate, and address, along with the signature of the consenting adult. Privacy is also a key component, with notifications regarding the rights to access and correct personal information collected by the state. Overall, this addendum not only facilitates the vaccination process but also ensures that informed consent is obtained, thereby promoting public health and safety in Texas.
| Fact Name | Description |
|---|---|
| Vaccine Type | The form is for the Tetanus and Diphtheria (Td) vaccine. |
| Consent Requirement | An adult must provide consent for the person receiving the vaccine. |
| Information Statement | A copy of the Vaccine Information Statement (VIS) must be provided to the individual. |
| Understanding Risks | The signer acknowledges understanding the risks of the disease and the vaccine. |
| Questions Allowed | Individuals are encouraged to ask questions about the vaccine and its administration. |
| Privacy Notification | Texas law allows individuals to request and review their personal information collected by the state. |
| HIPAA Compliance | Individuals must acknowledge receipt of the immunization provider’s HIPAA Privacy Notice. |
| Documentation | The form must be filed in the patient’s chart after being signed. |
| Governing Laws | Relevant laws include Government Code, Sections 552.021, 552.023, 559.003, and 559.004. |
Filling out the Texas Addendum to the Tdap Vaccine form is a straightforward process that ensures proper documentation for vaccination. After completing the form, it will be submitted to the appropriate health care provider or clinic. This helps maintain accurate records and ensures that the individual receives the necessary vaccine.
What is the Texas Addendum To Tdap Vaccine form?
The Texas Addendum To Tdap Vaccine form is a document that provides consent for an individual to receive the Tetanus and Diphtheria (Td) vaccine. It includes important information about the vaccine, the risks of the diseases it prevents, and the rights of the individual regarding their health information.
Who needs to fill out this form?
This form must be completed by an adult who can legally consent for the person receiving the vaccine. This could be a parent or guardian if the recipient is a minor. It is essential that the individual providing consent understands the information presented in the form.
What information is required on the form?
The form requires the name, birthdate, sex, and address of the person receiving the vaccine. Additionally, the signature of the person giving consent, along with the date, is necessary. This ensures that there is a clear record of consent for the vaccination.
What does the form indicate about the vaccine?
The form states that the individual understands the risks associated with the diseases that the vaccine prevents. It also confirms that they have been informed about the benefits and risks of receiving the vaccine. This ensures that informed consent is given.
What is the significance of the Privacy Notification?
The Privacy Notification informs individuals about their rights regarding personal information collected by the State of Texas. It emphasizes that individuals can request access to their information and can ask for corrections if any details are incorrect. This is important for maintaining personal privacy.
What should be done with the completed form?
Once the form is completed, it should be filed in the patient’s chart. This helps maintain accurate records of vaccinations and consent, which is crucial for future healthcare needs.
What if I have questions about the vaccine or the form?
If you have questions about the vaccine or the form itself, it is advisable to speak with a healthcare provider. They can provide detailed information and clarify any concerns you may have regarding the vaccination process.
Is there a specific website for more information?
Yes, more information can be found at the Texas Department of State Health Services website. This site provides additional resources regarding vaccines, health information, and privacy notifications.
What happens if the form is altered?
Altering or changing the Texas Addendum To Tdap Vaccine form is prohibited without written consent from the Texas Department of State Health Services. It is crucial to ensure that the form remains intact and unaltered to maintain its validity.
Incomplete Personal Information: One common mistake is failing to fill out all required fields for the person receiving the vaccine. Ensure that the name, birthdate, and address are complete and accurate. Missing information can lead to delays or issues in processing the vaccination.
Incorrect Signature: The form must be signed by the individual receiving the vaccine or an authorized person, such as a parent or guardian. Some individuals mistakenly sign in the wrong section or neglect to sign altogether, which can invalidate the consent.
Not Reviewing the Vaccine Information Statement: It is crucial to acknowledge that you have received or been offered the Vaccine Information Statement (VIS). Some people overlook this step, which is essential for understanding the benefits and risks associated with the vaccine.
Failure to Ask Questions: Individuals often forget to take advantage of the opportunity to ask questions about the vaccine. This can lead to misunderstandings about the vaccine's purpose and potential side effects. It is important to clarify any uncertainties before proceeding.
The Texas Addendum To Tdap Vaccine form is often accompanied by several other important documents. Each of these documents plays a crucial role in the vaccination process, ensuring that all necessary information is collected and that consent is properly obtained. Below is a list of commonly used forms alongside the Texas Addendum To Tdap Vaccine form.
These forms and documents work together to ensure a smooth vaccination process while safeguarding patient rights and health information. Properly completing and filing these documents is essential for compliance and effective patient care.
When filling out the Texas Addendum To Tdap Vaccine form, it is important to follow certain guidelines to ensure accuracy and compliance. Here are eight things you should and shouldn’t do:
Misconceptions about the Texas Addendum to Tdap Vaccine form can lead to confusion regarding vaccination processes and requirements. Here are eight common misconceptions:
Understanding these misconceptions can help individuals make informed decisions regarding vaccinations and the consent process.
Filling out the Texas Addendum To Tdap Vaccine form is an important step in ensuring that individuals receive the necessary immunizations. Here are some key takeaways to keep in mind:
By understanding these key points, individuals can ensure that they are well-prepared for the vaccination process and that all necessary steps are followed appropriately.