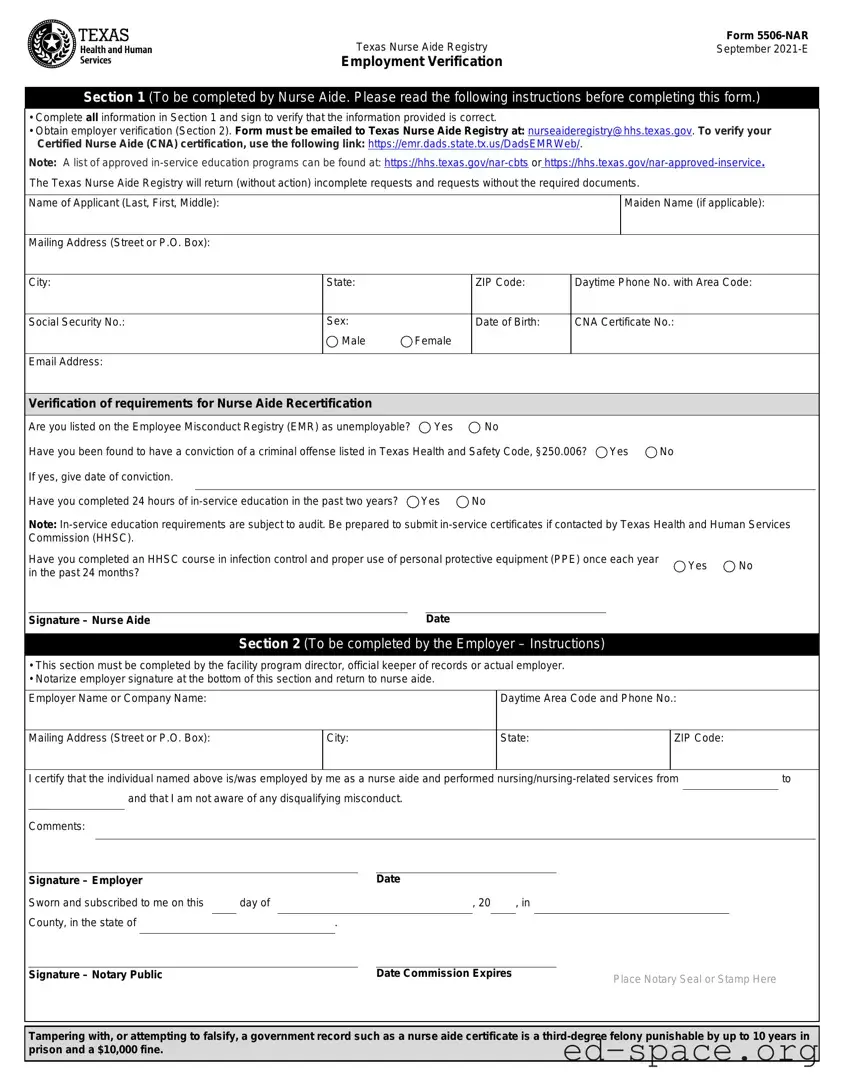
The Texas 5506 Nar form is a crucial document for individuals seeking to verify their employment as Certified Nurse Aides (CNAs) in Texas. It consists of two main sections that must be completed accurately to ensure successful processing. The first section is intended for the nurse aide, who must provide personal information, including their name, mailing address, and certification details. Additionally, the nurse aide must answer specific questions related to their employment history and compliance with in-service education requirements. This section requires the nurse aide's signature to confirm the accuracy of the information provided. The second section is designated for the employer, who must validate the nurse aide's employment and certify that no disqualifying misconduct has occurred. Notarization of the employer's signature is also a requirement, adding an extra layer of verification. It is important to note that incomplete forms or those lacking required documentation will be returned without action. For those looking to verify their CNA certification or obtain additional resources, links to the Texas Nurse Aide Registry and approved education programs are provided within the form. Understanding the significance of this form and the steps involved in its completion can greatly assist nurse aides in maintaining their certification and employment status.

| Fact Name | Description |
|---|---|
| Form Title | Texas Nurse Aide Registry Form 5506-NAR |
| Version Date | September 2021-E |
| Submission Method | The completed form must be emailed to [email protected]. |
| Employer Verification | Section 2 must be completed by the employer and notarized. |
| Criminal History Disclosure | Applicants must disclose any convictions listed in Texas Health and Safety Code, §250.006. |
| In-Service Education Requirement | Applicants must complete 24 hours of in-service education within the past two years. |
| Tampering Penalty | Falsifying records is a third-degree felony, punishable by up to 10 years in prison and a $10,000 fine. |
| Right to Information | Individuals can request to review and correct information held by the Texas Health and Human Services Commission (Government Code, Sections 552.021, 552.023, 559.004). |
Filling out the Texas 5506-NAR form is an essential step for nurse aides seeking recertification. Once completed, this form will be submitted to the Texas Nurse Aide Registry for processing. It's important to follow each step carefully to ensure that your application is complete and accurate.
After submitting the form, keep an eye on your email for any communication from the Texas Nurse Aide Registry. They may reach out for additional information or to confirm your recertification status. Make sure to retain copies of your submitted documents for your records.
What is the Texas 5506 Nar form?
The Texas 5506 Nar form, also known as the Nurse Aide Registry Form 5506-NAR, is a document required for verifying employment and recertification of Certified Nurse Aides (CNAs) in Texas. It consists of two sections: one for the nurse aide to complete and sign, and another for the employer to verify employment details. This form is essential for maintaining compliance with state regulations regarding nurse aide certification.
Who needs to fill out the Texas 5506 Nar form?
Any individual seeking to verify their employment as a nurse aide and maintain their certification in Texas must fill out this form. This includes CNAs who are recertifying their credentials and need to provide proof of their work history and completion of required in-service education hours.
What information is required in Section 1 of the form?
In Section 1, the nurse aide must provide personal details such as their name, mailing address, social security number, email address, and date of birth. They also need to indicate their CNA certificate number and answer questions regarding their employment history and compliance with in-service education requirements. Finally, the nurse aide must sign the form to verify that the information provided is accurate.
What does Section 2 entail?
Section 2 is to be completed by the employer. This section requires the employer to certify that the nurse aide was employed and performed nursing-related services during a specified time frame. The employer must also confirm that they are not aware of any disqualifying misconduct. After filling out this section, the employer's signature must be notarized to validate the information provided.
How do I submit the completed Texas 5506 Nar form?
Once both sections of the form are completed and signed, the nurse aide must email the form to the Texas Nurse Aide Registry at [email protected]. It is crucial to ensure that all information is accurate and that the employer's signature is notarized, as incomplete forms will be returned without action.
What happens if I do not meet the requirements for recertification?
If a nurse aide does not meet the recertification requirements, such as being listed on the Employee Misconduct Registry or failing to complete the required in-service education hours, they may be ineligible for recertification. It is essential to review all requirements carefully and ensure compliance to avoid any issues with certification status.
Where can I find additional resources related to the Texas 5506 Nar form?
Additional resources can be found on the Texas Health and Human Services website. This includes links to verify CNA certification status and access to approved in-service education programs. For any questions or further assistance, you can contact the Nurse Aide Registry at 512-438-2050.
Incomplete Information: Failing to fill out all sections of Section 1 can lead to delays. Ensure every required field is completed.
Missing Signature: Not signing Section 1 is a common oversight. Your signature is necessary to verify the accuracy of the information provided.
Employer Verification Issues: Section 2 must be completed by the employer. If this section is left blank or incorrectly filled out, it will delay processing.
Notarization Errors: The employer's signature in Section 2 must be notarized. Failing to do this can result in the form being returned.
Omitting Required Documents: If you do not include necessary documents with your submission, the Texas Nurse Aide Registry will return your request without action.
Incorrect Contact Information: Providing an incorrect email address or phone number can hinder communication regarding your application.
Not Checking Criminal History: If you have a conviction listed in Texas Health and Safety Code, it is essential to disclose this information accurately.
Ignoring In-Service Education Requirements: Ensure you have completed the required 24 hours of in-service education. Failing to do so may affect your recertification.
The Texas Nurse Aide Registry Form 5506-NAR is an essential document for individuals seeking to verify their status as Certified Nurse Aides (CNAs). However, several other forms and documents often accompany this application, ensuring a comprehensive review process. Below is a list of these additional documents, each playing a critical role in the verification and recertification process.
Each of these documents plays a vital role in ensuring that nurse aides meet the necessary requirements for certification and recertification. By providing a comprehensive set of information, applicants can facilitate a smoother review process, ultimately supporting their professional journey in the healthcare field.
The Texas 5506 Nurse Aide Registry Form is essential for verifying employment and certification for nurse aides. Similar forms serve comparable purposes in various professional contexts. Here are four documents that share similarities with the Texas 5506-NAR form:
When filling out the Texas 5506-NAR form, it is essential to follow certain guidelines to ensure your application is processed smoothly. Below is a list of things you should and shouldn't do:
By adhering to these guidelines, you can help ensure that your application for the Texas Nurse Aide Registry is handled efficiently and correctly.
This is incorrect. Section 2 of the form must be completed by the employer. Their verification is essential for the processing of the application.
This is not true. While the applicant completes Section 1, Section 2 requires input from the employer. Both sections are crucial for a valid submission.
This is misleading. The completed form must be emailed to the Texas Nurse Aide Registry. Other submission methods may not be accepted.
This is false. Completing 24 hours of in-service education in the past two years is a requirement for nurse aide recertification. Failure to meet this requirement can lead to complications in the recertification process.
Filling out the Texas 5506 Nar form is an important step for nurse aides. Here are some key takeaways to keep in mind:
By following these steps, you can ensure a smoother process in maintaining your certification as a nurse aide in Texas.