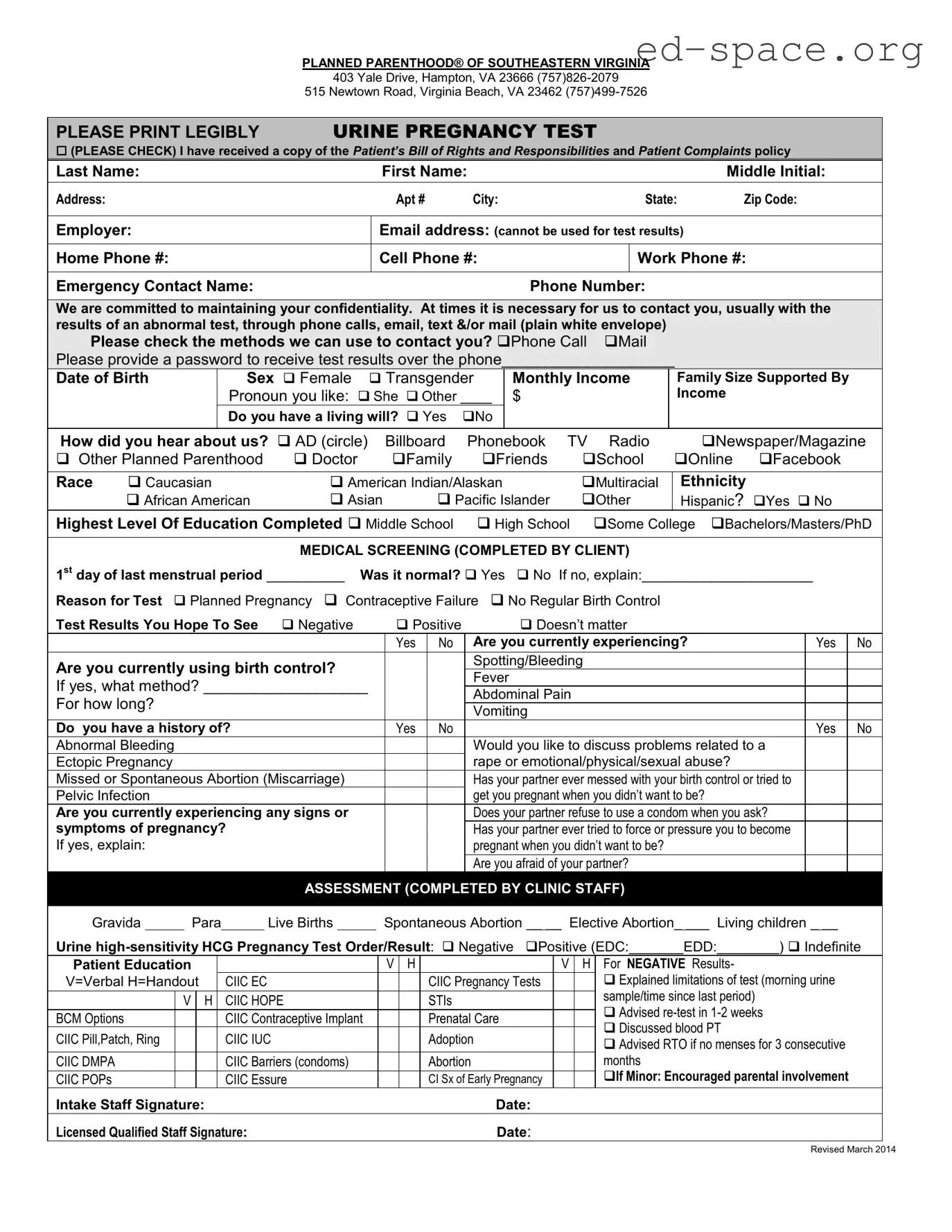
In today's world, where the intricacies of healthcare can often become overwhelming, understanding specific forms and procedures is crucial for individuals looking to navigate these systems effectively. The Planned Parenthood Proof form, utilized by Planned Parenthood of Southeastern Virginia, exemplifies this principle by serving as a comprehensive document that records a variety of vital information and consents relating to medical services and privacy practices. Key aspects of this form include clear instructions for patients to print legibly, checkboxes for the types of communication preferred, such as phone calls or mail, and sensitive questions about the patient’s health, sexual activity, and potential for pregnancy. It also delves into areas like a patient's medical history, contraception use, and even touches on sensitive topics such as domestic abuse, showcasing Planned Parenthood’s commitment to thorough patient care and confidentiality. Additionally, the form outlines the request for medical services and acknowledgment of receipt of Notice of Health Information Privacy Practices, ensuring that patients are fully informed about the kind of care they are consenting to and how their private information will be handled. This kind of form is vital in fostering an environment of trust and respect between healthcare providers and their patients, ultimately aiming to provide care that is both respectful and tailored to the individual's needs.
| Fact Name | Description |
|---|---|
| Organization Name | Planned Parenthood® of Southeastern Virginia |
| Locations | Hampton and Virginia Beach, Virginia |
| Form Purpose | Request for Medical Services and Acknowledgement of Receipt of Notice of Health Information Privacy Practices |
| Contact Methods | Patient consent is required for contact via phone calls, email, text, and/or mail for the communication of test results or necessary information. |
| Confidentiality Commitment | Planned Parenthood is dedicated to maintaining patient confidentiality as outlined in their Notice of Health Information Privacy Practices. |
| Governing Law(s) | Virginia state law, specifically regarding the requirement to report certain sexually transmitted infections to public health agencies. |
Completing the Planned Parenthood Proof form is a necessary step in accessing certain services provided by Planned Parenthood® of Southeastern Virginia. It's important to fill out the form accurately to ensure that the healthcare team can provide personalized and effective care. Here are the steps to fill out the form correctly:
After completing and submitting the form, the Planned Parenthood team will review your information and proceed with the necessary evaluations and treatments as requested. This process is a vital part of ensuring personalized care based on your specific needs and health information.
What is the Planned Parenthood Proof form used for?
This form is used to document and acknowledge the receipt of medical services and the understanding of health information privacy practices at Planned Parenthood of Southeastern Virginia. It includes sections for personal details, medical screening questions, and consent regarding health information privacy.
How can I provide my contact information safely?
You can indicate your preferred methods of contact, including phone calls and mail, on the form. Planned Parenthood is committed to maintaining confidentiality and advises checking the methods safe for you.
What should I do if I need a language interpreter?
Inform the staff if you require interpreter services for better understanding during your health care visits. Be aware that interpreter services may not be immediately available, and a referral to another facility might be necessary.
Can someone assist me in my care if I am a minor?
Yes, if you are a minor, Planned Parenthood encourages parental involvement and may require consent from a guardian depending on the services requested and state laws.
What happens if I change my mind about receiving medical services?
You have the right to change your mind about receiving services at any time. Your choice will be respected and you can discontinue services as per your decision.
Is the information I provide guaranteed to be confidential?
Yes, Planned Parenthood assures that all information provided will be kept confidential as outlined in their Notice of Health Information Privacy Practices.
What happens if my tests for sexually transmitted infections are positive?
If tests for certain sexually transmitted infections are positive, reporting to public health agencies is required by law. You will also receive referrals for further diagnosis or treatment if necessary.
Who can sign the form if the patient is not able to?
If the patient is unable to sign for themselves, a guardian or relative legally required to consent can sign the form on the patient's behalf. Their relationship to the patient must be noted on the form along with a witness signature.
How do I acknowledge receipt of Planned Parenthood’s Notice of Health Information Privacy Practices?
By signing the form, you acknowledge that you have received and understood the Notice of Health Information Privacy Practices provided by Planned Parenthood Southeastern Virginia.
What should I do if I have any questions about the form or the services?
You should ask questions about anything you do not understand before signing the form. A clinician or staff member at Planned Parenthood will be happy to discuss any concerns or questions you may have about the form, the services, or your rights as a patient.
When filling out the Planned Parenthood Proof form, people can make several common mistakes that may impact the processing of their form or the care they receive. It is crucial to avoid these errors to ensure accurate and efficient service.
By avoiding these common mistakes and ensuring all sections of the form are completed accurately and thoroughly, individuals can help Planned Parenthood provide the best possible care tailored to their specific needs.
When individuals utilise the Planned Parenthood Proof form, they are often engaging with a larger framework of healthcare services. This form is a crucial piece in ensuring individuals receive the comprehensive care they need, respecting their privacy and personal choices throughout the process. To support this, several other forms and documents may accompany the Planned Parenthood Proof form to provide a holistic approach to healthcare and administrative procedures.
Together, these forms and documents ensure that patients are well-informed, their privacy is respected, and they receive the personalized care they deserve. The integration of these documents into patient care processes represents the comprehensive approach to healthcare that organizations like Planned Parenthood strive to provide. Ensuring patients' understanding and consent, safeguarding their health information, and addressing their financial concerns are all essential aspects of delivering quality healthcare services.
Medical Consent Forms: Similar to the Planned Parenthood Proof form, medical consent forms often gather personal information, including contact details, medical history, and consent for medical services and treatments. Both types of documents aim to ensure that patients understand the treatments or tests they will undergo and consent to them.
Patient Registration Forms: These forms, like the Planned Parenthood Proof form, collect demographic information such as name, address, and employment details. They are designed to record patient information at healthcare facilities for future communication and billing purposes.
Notice of Privacy Practices Acknowledgement Forms: Similar to sections of the Planned Parenthood Proof form, these documents outline how a patient's health information will be used and protected. They ensure that patients are aware of their privacy rights regarding personal health information.
Emergency Contact Forms: These forms, also part of the Planned Parenthood Proof document, collect information on whom to contact in an emergency. Both types of forms prioritize patient safety and preparedness for any urgent situations.
Informed Consent for Treatment Forms: Much like the Planned Parenthood document, these forms require patients to acknowledge that they have been informed about the benefits and risks of a specific treatment or procedure and consent to it. This process is fundamental in healthcare to ensure ethical and legal compliance.
Health Screening Questionnaires: These questionnaires, partially mirrored in the Planned Parenthood Proof form, collect information on a patient’s recent health history, symptoms, and concerns. They are used to assess the patient's current health status and determine necessary medical interventions.
Sexual Health History Forms: Similar to elements within the Planned Parenthood Proof document, these forms gather sensitive information related to sexual health and practices. They help healthcare providers offer appropriate care, advice, and treatment options related to sexual health.
When filling out the Planned Parenthood Proof form, it is essential to ensure that the process is done accurately and thoughtfully. Below are six things you should do and six things you shouldn't do to ensure the form is completed correctly.
Things You Should Do:
Things You Shouldn't Do:
Planned Parenthood provides a range of healthcare services and aims to ensure patient understanding and confidentiality throughout the care process. However, misconceptions about the Planned Parenthood Proof form and the organization's practices can often mislead or confuse individuals seeking care. Below, we discuss and clarify four common misconceptions:
Patients often believe that consent to treatment at Planned Parenthood facilities is automatically assumed. This is not accurate. The Planned Parenthood Proof form explicitly requires patients to acknowledge and sign, indicating their informed consent before receiving any medical services or treatments. This process ensures that patients are fully aware of the nature of the healthcare services provided, including the associated benefits, risks, and alternate choices available to them.
Some individuals mistakenly think that their personal information and treatment details might be easily accessed or disclosed without their consent. Contrary to this belief, Planned Parenthood is deeply committed to maintaining patient confidentiality. The organization adheres to strict privacy policies, as outlined in their Notice of Health Information Privacy Practices, which is acknowledged and signed by the patient. This document confirms that all personal health information is treated with the utmost confidentiality and is only shared in compliance with applicable laws and with patient consent.
A common misconception is that Planned Parenthood's services are exclusively for women. However, Planned Parenthood offers a wide range of health care services to individuals of all genders, including men and transgender people. The Planned Parenthood Proof form asks about sex and preferred pronouns, acknowledging and respecting the gender diversity of their patients and catering to the healthcare needs of a broad patient demographic.
Another common misunderstanding is that individuals without health insurance cannot receive immediate medical services from Planned Parenthood. In reality, Planned Parenthood is dedicated to providing care to all individuals, regardless of their insurance status or ability to pay. The organization offers sliding scale fees based on an individual's income and family size to ensure that everyone has access to the healthcare services they require. This commitment is part of their mission to provide comprehensive and accessible reproductive health care and education.
Filling out the Planned Parenthood Proof form is an essential step for individuals seeking medical services and acknowledging privacy practices at Planned Parenthood of Southeastern Virginia. Below are key takeaways to guide individuals through the process:
Completion of the Planned Parenthood Proof form signifies a patient's informed consent to receive services, along with an understanding of their rights and the privacy practices in place to protect their health information. It's a vital part of ensuring quality care and support for individuals utilizing Planned Parenthood’s services.
Georgia New Hire - The Georgia New Hire Reporting Form is required for all employers in the state.
Statement of Information Vs Articles of Organization - If your LLP is foreign and has changed its name, include a certificate from your home jurisdiction.
Can You Spare a Dollar Fundraiser Sheet - Your generosity is greatly appreciated.