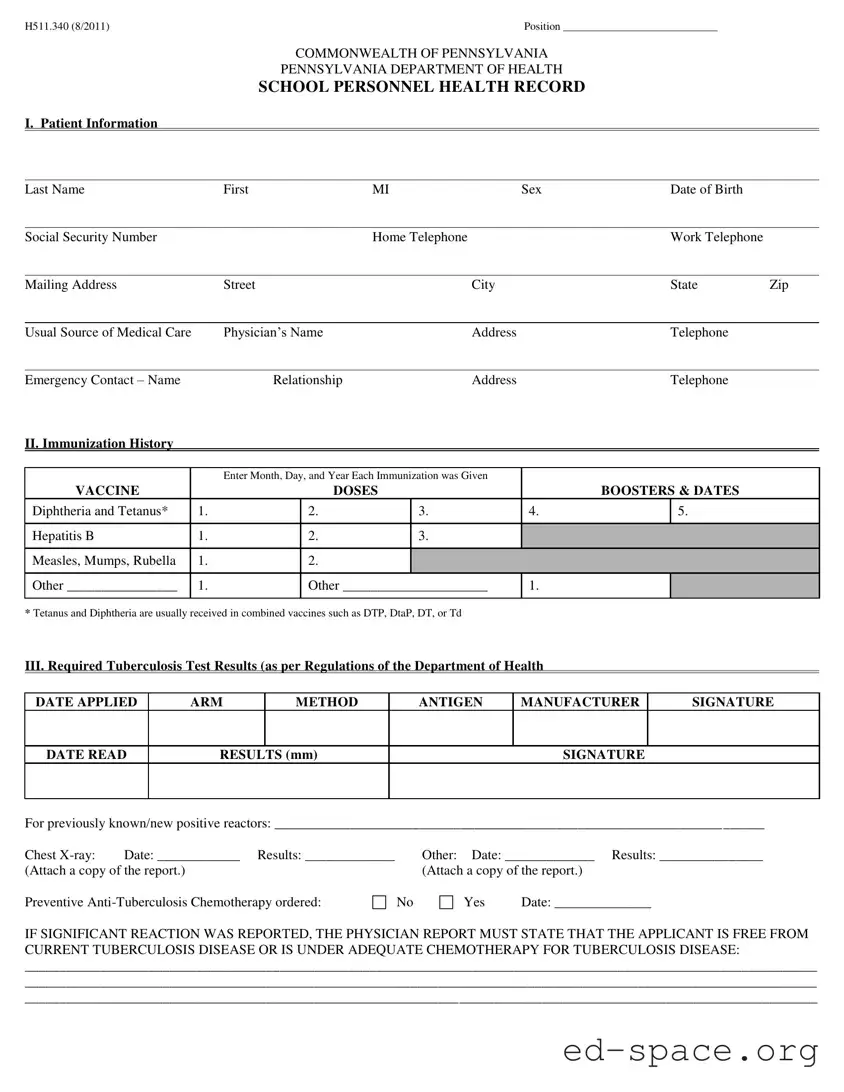
The Pennsylvania Health form, officially known as the School Personnel Health Record, is a vital document designed to ensure the health and safety of school personnel. This form collects essential patient information, including personal details such as name, date of birth, and contact information, alongside the individual's usual source of medical care. Immunization history is a significant section, where records of vaccinations like Diphtheria, Tetanus, Hepatitis B, and Measles, Mumps, and Rubella must be documented. Tuberculosis test results are also mandatory, requiring specific details about the testing method, results, and any necessary follow-up actions. The form further addresses significant medical conditions, allowing for transparency regarding allergies, chronic illnesses, and other health concerns that may impact an individual's ability to perform their duties. A thorough physical examination report is included, which assesses various health metrics and identifies any special medical issues that could necessitate activity restrictions. Completing this form accurately is crucial, as it not only affects employment eligibility but also plays a role in maintaining a healthy school environment.
| Fact Name | Description |
|---|---|
| Governing Law | The Pennsylvania Health Form is governed by the Pennsylvania Department of Health regulations. |
| Form Version | This form is identified as H511.340 and was last updated in August 2011. |
| Purpose | The form serves as a health record for school personnel in Pennsylvania. |
| Patient Information | It collects essential personal details such as name, date of birth, and contact information. |
| Immunization History | The form requires a detailed record of immunizations, including vaccines and booster dates. |
| Tuberculosis Testing | Results of tuberculosis tests must be documented as per the Department of Health regulations. |
| Medical Conditions | It includes a section for reporting significant medical conditions and allergies. |
| Physical Examination Report | A physical examination section records various health metrics and observations. |
Completing the Pennsylvania Health form requires careful attention to detail. Each section must be filled out accurately to ensure that all necessary information is provided. Once you have completed the form, you will need to submit it to the appropriate authority as part of your health record requirements.
What is the purpose of the Pennsylvania Health Form?
The Pennsylvania Health Form is designed to collect essential health information about school personnel. This information helps ensure that employees are physically capable of performing their job duties and that any health issues are documented. It includes sections on immunization history, tuberculosis test results, significant medical conditions, and a report of physical examination. Completing this form accurately is crucial for maintaining a safe and healthy school environment.
Who is required to complete the Pennsylvania Health Form?
All school personnel in Pennsylvania, including teachers, administrators, and support staff, must complete the Pennsylvania Health Form. This requirement is in place to comply with state health regulations and to promote the well-being of both employees and students. New hires typically need to submit this form before starting work, while current employees may be asked to update their information periodically.
What should I do if I have a significant medical condition?
If you have a significant medical condition, it is important to disclose this information on the Pennsylvania Health Form. The form includes a section where you can indicate any allergies, chronic illnesses, or other health issues that may affect your work. Being transparent about your health helps ensure that appropriate accommodations can be made if necessary. If you have concerns about privacy, rest assured that this information is handled confidentially and is only shared with authorized personnel.
What happens if I do not complete the Pennsylvania Health Form?
Failure to complete the Pennsylvania Health Form may result in delays in your employment process or even termination of your employment. The form is a crucial part of ensuring that all school personnel meet health and safety standards. It is advisable to fill out the form thoroughly and return it promptly to avoid any issues. If you have questions or need assistance, reach out to your employer for guidance.
Missing Personal Information: Not providing complete personal details like last name, first name, or date of birth can lead to processing delays.
Incorrect Social Security Number: Entering an incorrect Social Security number can create significant issues with identification and benefits.
Incomplete Immunization History: Failing to list all vaccinations or not including the dates can result in non-compliance with health regulations.
Skipping Tuberculosis Test Details: Not providing the date applied, method, or results of the tuberculosis test can lead to rejection of the form.
Omitting Significant Medical Conditions: Not disclosing allergies or other medical conditions can affect job performance and safety.
Not Signing the Form: Forgetting to sign the form at the end can render it invalid.
Ignoring Required Attachments: Failing to attach necessary reports, such as chest X-ray results, can delay processing.
Inaccurate Emergency Contact Information: Providing incorrect contact details can hinder communication in case of an emergency.
Neglecting to Update Information: Not updating any changes in health status or personal information can lead to complications later.
Forgetting to Review the Form: Not double-checking for errors or omissions before submission can cause unnecessary delays and issues.
When completing the Pennsylvania Health form, you may also need to gather additional documents to ensure a comprehensive health record. Here are some commonly used forms that can complement the Pennsylvania Health form:
Gathering these documents alongside the Pennsylvania Health form can help create a complete health profile. This ensures that all necessary information is readily available for schools or employers, streamlining the process and enhancing safety and compliance.
The Pennsylvania Health form is an essential document for school personnel, ensuring that health information is accurately recorded and accessible. Several other documents serve similar purposes in various contexts, focusing on health history, immunizations, and medical evaluations. Here are five documents that share similarities with the Pennsylvania Health form:
Each of these documents plays a vital role in maintaining health records, ensuring safety, and promoting well-being in various environments. Understanding their similarities can help individuals navigate health-related requirements more effectively.
When filling out the Pennsylvania Health form, it’s important to approach the task with care and attention to detail. Here’s a list of ten things you should and shouldn’t do to ensure your submission is accurate and complete.
By following these guidelines, you can help ensure that your Pennsylvania Health form is completed correctly, making the process smoother for everyone involved.
Understanding the Pennsylvania Health form is crucial for compliance and proper documentation. However, several misconceptions can lead to confusion. Here are four common misconceptions:
While the form is titled "School Personnel Health Record," it is applicable to various roles within educational settings. Any employee or volunteer who interacts with students may need to complete this form to ensure health and safety standards are met.
Immunization history is a required section of the form. Accurate documentation of vaccinations is essential for preventing outbreaks of contagious diseases in schools and ensuring the health of all students and staff.
The form mandates tuberculosis testing regardless of symptom presence. This requirement is in place to safeguard public health, especially in environments where individuals are in close contact.
While a physician must review and sign the form, other qualified health professionals, such as nurse practitioners or physician assistants, may also complete the examination and documentation. This flexibility can streamline the process for employees.
Ensure all patient information is filled out accurately. This includes your name, date of birth, and contact details.
List your usual source of medical care, including the physician’s name and contact information.
Document your immunization history clearly. Provide the dates for each vaccine received.
Complete the Tuberculosis test results section as required. Include the date applied and the results.
Indicate any significant medical conditions by checking the appropriate boxes. Provide explanations where necessary.
Ensure the physical examination report is filled out completely. This includes height, weight, and any abnormalities.
Read through the form carefully before submission to ensure all sections are complete and accurate.
Sign and date the form at the bottom to confirm that all information is true to the best of your knowledge.
Keep a copy of the completed form for your records after submission.