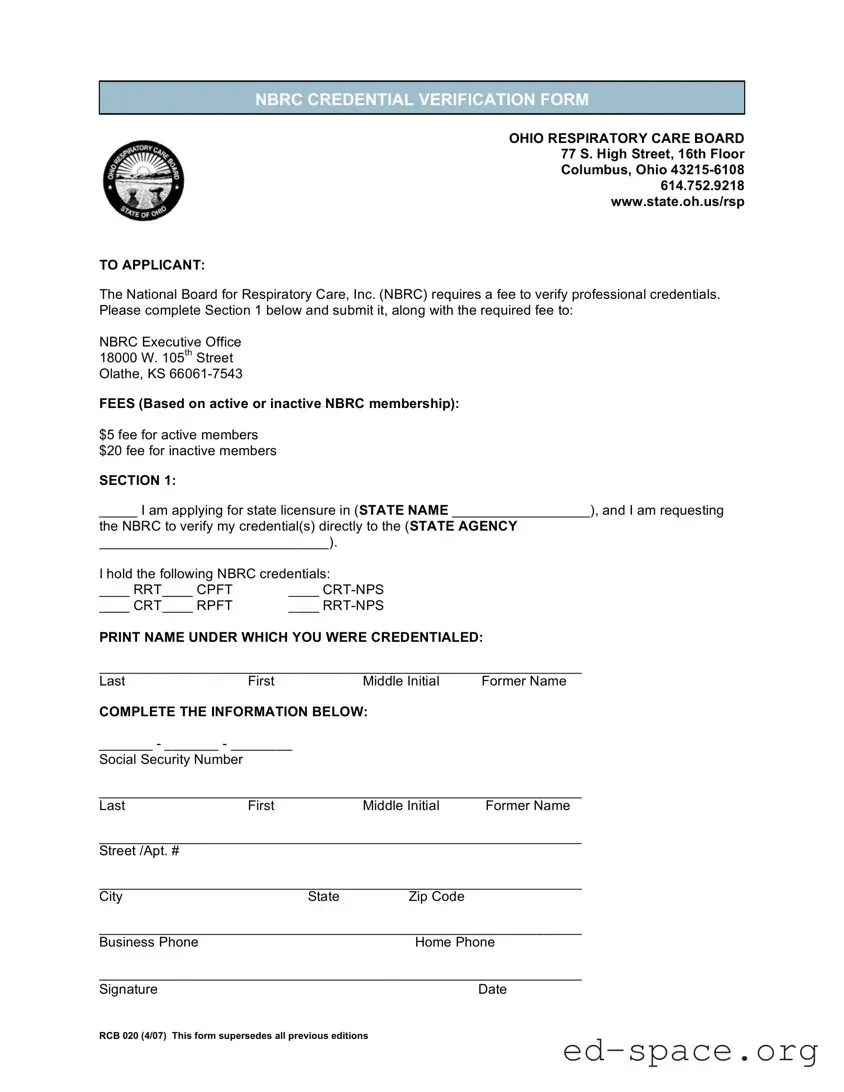
The Ohio RCB 020 form is a crucial document for individuals seeking state licensure in respiratory care. It serves as a credential verification form required by the National Board for Respiratory Care (NBRC). Applicants must complete the form to facilitate the verification of their professional credentials directly to the relevant state agency. The form includes essential sections where applicants provide their personal information, including their name, Social Security number, and contact details. Additionally, it specifies the required fees for processing the verification, which vary based on the applicant's NBRC membership status. Active members pay a fee of $5, while inactive members are required to pay $20. This form not only streamlines the licensure process but also ensures that the credentials of respiratory care professionals are accurately verified, thereby maintaining the standards of the profession in Ohio.
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The Ohio RCB 020 form is used for credential verification by the National Board for Respiratory Care (NBRC) for individuals applying for state licensure in Ohio. |
| Governing Body | The form is governed by the Ohio Respiratory Care Board. |
| Fee Structure | Active NBRC members pay a fee of $5, while inactive members pay $20 for credential verification. |
| Submission Address | Completed forms must be sent to the NBRC Executive Office in Olathe, Kansas. |
| Contact Information | The Ohio Respiratory Care Board can be contacted at 614.752.9218 for inquiries related to the form. |
| Applicant Information | Applicants must provide their name, social security number, and contact information on the form. |
| Credential Types | Applicants can hold various NBRC credentials, including RRT, CPFT, CRT-NPS, CRT, RPFT, and RRT-NPS. |
| Signature Requirement | A signature and date are required from the applicant to validate the form. |
| Edition Date | The current edition of the RCB 020 form was last updated in April 2007 and supersedes all previous editions. |
Completing the Ohio RCB 020 form is a straightforward process. This form is essential for verifying your professional credentials with the National Board for Respiratory Care (NBRC). Once you fill it out, you will need to submit it along with the required fee to the designated address.
What is the Ohio RCB 020 form?
The Ohio RCB 020 form is a credential verification form required by the National Board for Respiratory Care (NBRC) for individuals applying for state licensure in Ohio. It facilitates the verification of professional credentials directly to the appropriate state agency.
Who needs to fill out the Ohio RCB 020 form?
Any applicant seeking licensure as a respiratory care professional in Ohio must complete this form. This includes individuals holding various NBRC credentials such as RRT, CRT, CPFT, and others.
What fees are associated with the Ohio RCB 020 form?
There are fees based on your NBRC membership status. Active members pay a fee of $5, while inactive members are required to pay $20. This fee is necessary for the NBRC to process the credential verification.
Where should I send the completed Ohio RCB 020 form?
Once you have completed the form and included the required fee, send it to the NBRC Executive Office at 18000 W. 105th Street, Olathe, KS 66061-7543. Ensure all sections are filled out accurately to avoid delays.
What information do I need to provide on the form?
You will need to provide your personal information, including your full name (and any former names), Social Security number, contact details, and the specific NBRC credentials you hold. Make sure to double-check all entries for accuracy.
Is there a deadline for submitting the Ohio RCB 020 form?
While there is no specific deadline mentioned for the form submission, it is advisable to submit it as soon as possible to ensure that your credential verification is completed in a timely manner. Check with the Ohio Respiratory Care Board for any specific timelines related to your licensure application.
What should I do if I have questions about the Ohio RCB 020 form?
If you have questions or need assistance while filling out the Ohio RCB 020 form, you can contact the Ohio Respiratory Care Board at 614.752.9218. They can provide guidance and help clarify any uncertainties you may have.
Incomplete Personal Information: Many applicants forget to fill in all required personal details, such as their full name, social security number, and contact information. This can lead to delays in processing.
Incorrect Fee Submission: Submitting the wrong fee based on membership status is a common mistake. Active members should pay $5, while inactive members need to submit $20. Double-check your membership status before sending the payment.
Omitting the State Name: Failing to specify the state for licensure can halt the application process. Ensure you clearly indicate the state in the designated area of the form.
Neglecting to Sign and Date: Some applicants forget to sign and date the form. Without a signature, the application may be considered incomplete.
Incorrectly Listing Credentials: Applicants often misidentify their NBRC credentials. It’s crucial to accurately check the boxes for the credentials you hold to avoid confusion.
Failure to Review Before Submission: Rushing through the form can lead to overlooked errors. Taking a moment to review the entire form before sending it can save time and prevent issues.
The Ohio RCB 020 form is essential for individuals seeking licensure in respiratory care within Ohio. However, several other forms and documents are often used in conjunction with it to ensure a smooth application process. Below is a list of these documents, each playing a vital role in the licensure journey.
Each of these documents serves a specific purpose in the licensure process, contributing to a comprehensive evaluation of the applicant's qualifications and readiness to practice respiratory care in Ohio. Properly completing and submitting these forms can facilitate a more efficient review by the Ohio Respiratory Care Board.
The Ohio RCB 020 form, utilized for credential verification by the National Board for Respiratory Care (NBRC), shares similarities with several other important documents in the healthcare and licensing fields. Understanding these documents can provide clarity and streamline the application process for professionals seeking licensure or credential verification. Here are nine documents that are similar to the Ohio RCB 020 form:
Understanding these forms can aid applicants in navigating the complex landscape of professional licensure and credential verification. Each document plays a crucial role in ensuring that healthcare professionals meet the necessary standards for practice.
When filling out the Ohio RCB 020 form, attention to detail is crucial. Below is a list of important dos and don'ts to guide you through the process.
By following these guidelines, you can help ensure that your application process goes smoothly and that your credentials are verified without unnecessary delays.
Understanding the Ohio RCB 020 form is essential for applicants seeking licensure. However, several misconceptions can lead to confusion. Here are eight common misunderstandings:
By clarifying these misconceptions, applicants can navigate the licensure process more effectively and avoid unnecessary delays.
Filling out the Ohio RCB 020 form is a crucial step for applicants seeking licensure in respiratory care. Here are some key takeaways to ensure you navigate the process smoothly:
By paying attention to these details, you can help ensure a smoother application process and avoid potential setbacks. Take action now to secure your future in respiratory care.