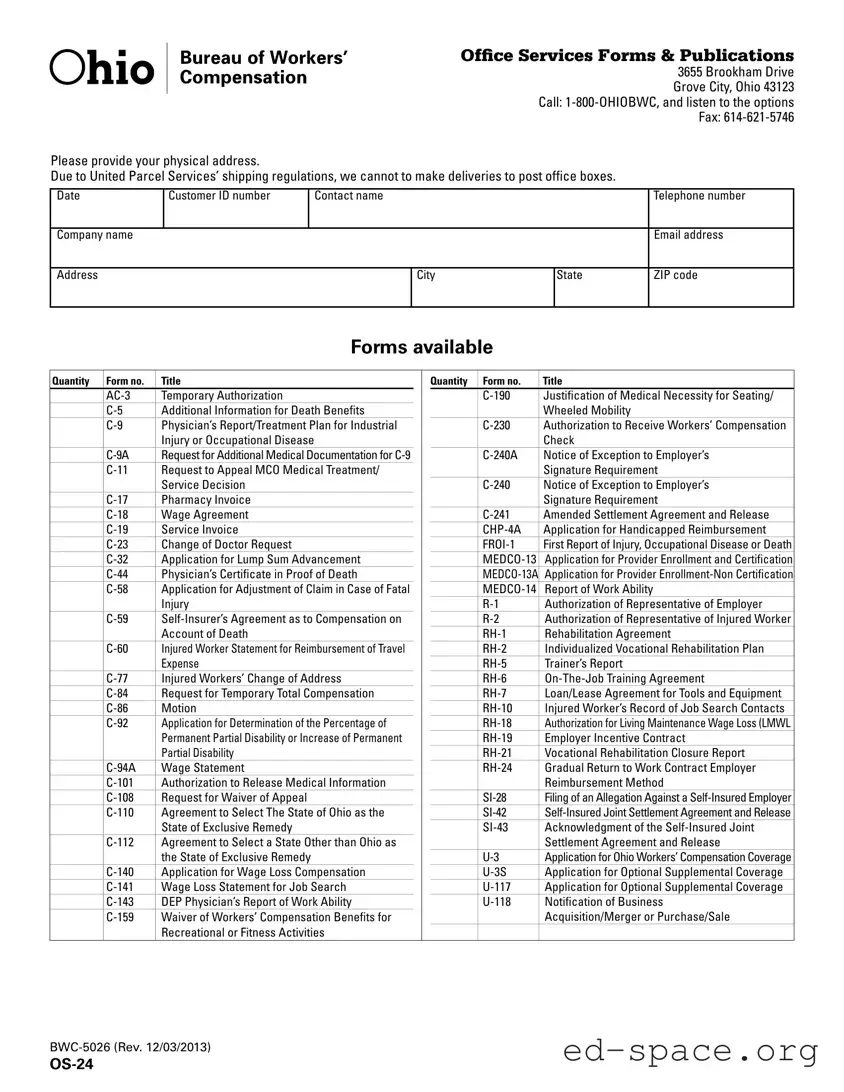
The Ohio OS-24 form serves as a comprehensive resource for individuals and businesses seeking various forms and publications related to workers' compensation and safety in Ohio. This form includes essential information such as the customer ID number, contact details, and physical address, which is crucial for processing requests. Notably, it outlines a wide array of available forms, including applications for wage loss compensation, requests for medical documentation, and reports of work ability. Additionally, the OS-24 form provides access to important publications, such as fraud brochures and safety posters, aimed at educating stakeholders about their rights and responsibilities. Users must note that certain forms are not available through the Bureau of Workers' Compensation (BWC) and should contact the Industrial Commission of Ohio for those specific needs. By centralizing this information, the OS-24 form streamlines the process for obtaining necessary documentation and enhances compliance with Ohio’s workers' compensation regulations.
| Fact Name | Details |
|---|---|
| Purpose | The OS-24 form is used to request various forms and publications related to workers' compensation services in Ohio. |
| Contact Information | Individuals can reach the Ohio Bureau of Workers' Compensation by calling 1-800-OHIOBWC or by faxing at 614-621-5746 for assistance. |
| Physical Address Requirement | Due to shipping regulations, the form requires a physical address for delivery, as post office boxes are not accepted. |
| Available Forms | The OS-24 form provides a list of various forms available for different workers' compensation needs, including applications for benefits and reports. |
| Governing Law | The OS-24 form is governed by the Ohio Revised Code, specifically Title 4123, which pertains to workers' compensation laws in Ohio. |
Completing the Ohio OS-24 form is a straightforward process that requires attention to detail. This form is essential for requesting various forms and publications related to workers' compensation. Properly filling it out ensures that you receive the necessary materials in a timely manner.
What is the Ohio OS 24 form?
The Ohio OS 24 form is a document used to request various forms and publications related to workers' compensation in Ohio. It serves as a means for individuals or organizations to obtain necessary paperwork from the Bureau of Workers' Compensation (BWC).
How can I submit the Ohio OS 24 form?
You can submit the Ohio OS 24 form by providing your physical address and contact information. Due to shipping regulations, deliveries cannot be made to post office boxes. The completed form can be sent via fax to 614-621-5746 or by contacting the BWC office directly.
What information do I need to provide on the OS 24 form?
When filling out the OS 24 form, you need to provide your customer ID number, contact name, telephone number, company name, email address, and physical address, including city, state, and ZIP code. This information is essential for processing your request accurately.
What types of forms are available through the OS 24 form?
The OS 24 form allows you to request a variety of forms related to workers' compensation, including but not limited to the AC-3 Temporary Authorization, C-5 Additional Information for Death Benefits, and C-84 Request for Temporary Total Compensation. A complete list of available forms is included with the OS 24 form.
Is there a limit to the number of forms I can request?
There is no specified limit to the number of forms you can request using the OS 24 form. However, it is advisable to only request forms that you genuinely need to ensure efficient processing.
Who should I contact if I have questions about the OS 24 form?
If you have questions regarding the OS 24 form or the forms available through it, you can call the BWC at 1-800-OHIOBWC. This hotline provides options for assistance and information related to workers' compensation.
Can I obtain Industrial Commission of Ohio forms through the OS 24 form?
No, the OS 24 form is specifically for requesting BWC forms and publications. If you need forms from the Industrial Commission of Ohio, you must call their forms and publications number at 614-644-8009.
What should I do if I need a form that is not listed on the OS 24 form?
If you require a form that is not listed on the OS 24 form, it is recommended to contact the BWC office directly for guidance. They may provide alternative solutions or direct you to the appropriate resources for obtaining the necessary forms.
Failing to provide a physical address instead of a post office box. The form explicitly states that deliveries cannot be made to P.O. boxes, which can lead to delays in receiving important documents.
Omitting the Customer ID number. This number is crucial for processing the form accurately and efficiently.
Incorrectly filling out the contact information. This includes providing an inaccurate telephone number or email address, which can hinder communication.
Not specifying the quantity of forms requested. Each form needs to be clearly indicated to ensure the correct number is supplied.
Leaving out the company name. This is essential for identifying the entity associated with the request and can cause confusion.
Failing to include the date on the form. Without a date, it may be difficult to track the timeline of requests and submissions.
Using incorrect or outdated form numbers. Each form has a specific number, and using an incorrect one can lead to processing errors.
Not signing or dating the form where required. A missing signature can render the form invalid and delay processing.
The Ohio OS-24 form is a key document used in the workers' compensation process in Ohio. It is often accompanied by various other forms that serve specific purposes related to claims, medical documentation, and appeals. Below is a list of additional forms and documents commonly used alongside the OS-24 form.
Each of these forms plays a vital role in ensuring that the workers' compensation process runs smoothly and that all necessary information is collected for effective claims management. Proper use of these documents can significantly impact the outcome of a claim or appeal.
The Ohio OS-24 form serves as a resource for various forms and publications related to workers' compensation. Several other documents share similarities with the OS-24 form in terms of purpose, structure, or the information they require. Here’s a list of eight documents that are comparable to the OS-24 form:
When filling out the Ohio OS-24 form, it’s important to follow some key guidelines. Here are four things you should and shouldn’t do:
Misconceptions about the Ohio OS-24 form can lead to confusion regarding its purpose and usage. Here are seven common misconceptions:
Understanding these misconceptions can help individuals navigate the workers' compensation system in Ohio more effectively.
Filling out the Ohio OS-24 form can be straightforward if you keep a few key points in mind. Here are some important takeaways to help you navigate the process:
By keeping these points in mind, you can fill out the Ohio OS-24 form effectively and ensure that your workers' compensation needs are addressed promptly.