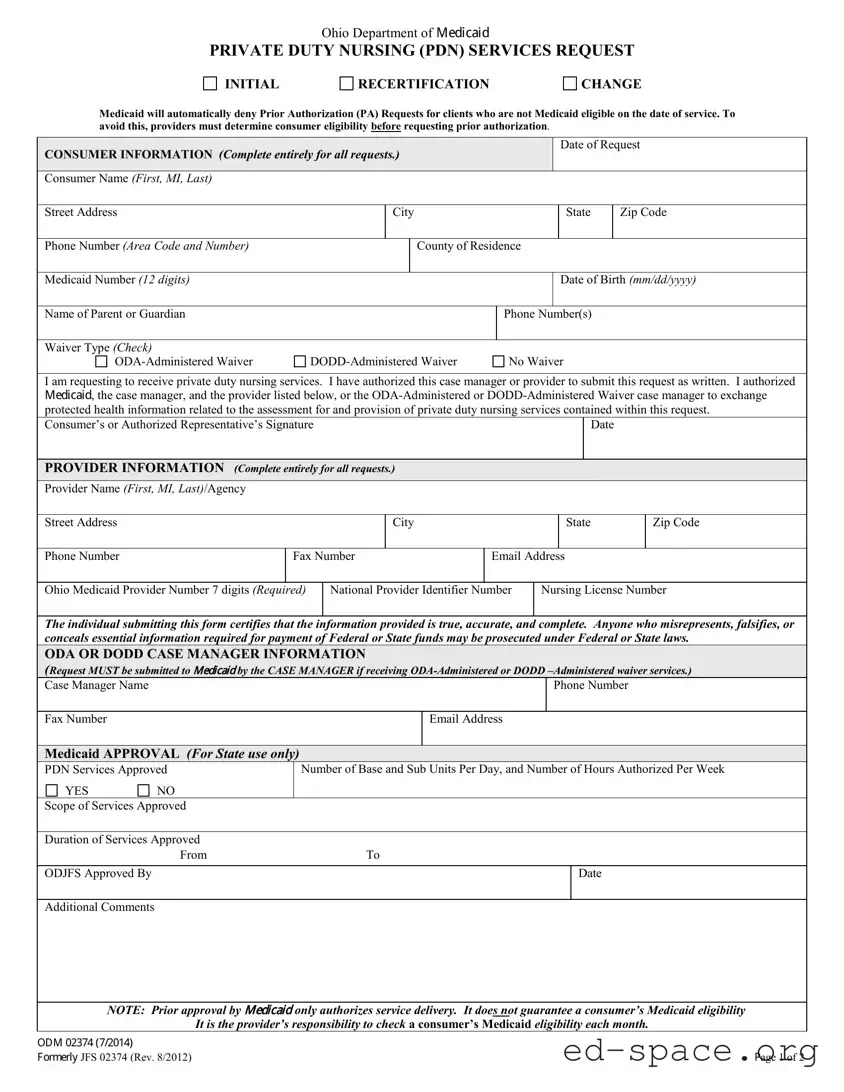
The Ohio ODM 02374 form plays a crucial role in the request process for Private Duty Nursing (PDN) services under Medicaid. Designed for both initial requests and recertifications, this form ensures that consumers receive the necessary nursing care while adhering to the regulations set forth by the Ohio Department of Medicaid. Before submitting a request, providers must confirm the consumer's Medicaid eligibility, as any requests made for ineligible clients will be automatically denied. The form collects essential consumer information, such as the individual's name, address, Medicaid number, and date of birth, as well as details about the parent or guardian if applicable. Providers must also include their information, including their Ohio Medicaid Provider Number and National Provider Identifier. Notably, the form requires a signature from the consumer or their authorized representative, granting permission for the case manager or provider to exchange health information pertinent to the request. Additionally, there are sections dedicated to documenting emergency services, changes in service requests, and the necessary physician’s letter when requesting PDN services beyond the standard 60-day post-hospital benefit. Understanding the intricacies of the ODM 02374 form is vital for both providers and consumers to navigate the complexities of Medicaid services effectively.

| Fact Name | Details |
|---|---|
| Form Purpose | The ODM 02374 form is used to request private duty nursing (PDN) services, including initial requests, recertifications, and changes in services. |
| Eligibility Check | Providers must confirm Medicaid eligibility before submitting a prior authorization request to avoid automatic denial. |
| Consumer Information | Complete consumer details are required, including name, address, Medicaid number, and guardian information, if applicable. |
| Provider Information | Providers must fill out their details, including their Medicaid provider number and nursing license number, to ensure proper processing. |
| Governing Law | The form is governed by Ohio Administrative Code (OAC) 5101:3-12-02.3 and OAC 5101:3-1-01. |
| Emergency Services | PDN services can be provided in emergencies, but a notification must be submitted by the next business day following service provision. |
| Submission Guidelines | All requests must be submitted via the Medicaid MITS Web Portal; faxes or emails are not accepted for PDN requests. |
Completing the Ohio ODM 02374 form is essential for requesting private duty nursing services. It is important to ensure that all sections are filled out accurately to avoid delays in processing. After submitting the form, the request will be reviewed, and a determination will be made regarding the authorization of services.
What is the Ohio ODM 02374 form used for?
The Ohio ODM 02374 form is a request for Private Duty Nursing (PDN) services. It is used to initiate, recertify, or change the services provided to Medicaid recipients who require additional nursing care. This form ensures that the necessary information is collected to assess eligibility and authorize the required nursing services.
Who needs to fill out the ODM 02374 form?
The form must be completed by the consumer or their authorized representative, as well as the provider of the nursing services. If the consumer is enrolled in an ODA-Administered or DODD-Administered waiver, the case manager must also submit the form. Accurate completion of the form is essential to avoid delays in service provision.
What information is required on the form?
The form requires detailed consumer information, including the consumer's name, address, Medicaid number, date of birth, and the name of the parent or guardian if applicable. Additionally, provider information, including the provider's name, address, and Medicaid provider number, must be included. A signature from the consumer or their authorized representative is also necessary to authorize the request.
How does one check Medicaid eligibility before submitting the form?
Providers must verify the consumer's Medicaid eligibility before submitting the ODM 02374 form. This step is crucial because Medicaid will automatically deny prior authorization requests for clients who are not eligible on the date of service. Providers can check eligibility through the Ohio Medicaid MITS Web Portal or by contacting the appropriate Medicaid office.
What should be included if requesting PDN services beyond the standard 60-day benefit?
If a consumer requires PDN services beyond the 60-day post-hospital benefit, a signed letter from the attending physician is needed. This letter should detail the current diagnosis, history of the illness, projected discharge date, and the estimated frequency and duration of the required services. It should also specify the expected skilled nursing interventions.
What happens if emergency PDN services are provided?
In cases where emergency PDN services are provided, a notification must be submitted no later than the first business day following the service. The notification should include the reason for the emergency, the number of service units provided, and the duration of the service. This ensures that the services are documented and can be authorized appropriately.
Can changes to services be requested using the ODM 02374 form?
Yes, the form can be used to request changes in services, including increases, decreases, terminations, or withdrawals. When requesting a change, it is important to provide details about the current and requested services, along with a justification for the change, such as physician orders or visit notes.
How should the completed form be submitted?
The completed ODM 02374 form must be submitted via the Medicaid MITS Web Portal. It is important to note that faxes or emails are not accepted for PDN requests. However, for DODD Service Coordinators and PASSPORT Case Managers, the form can be emailed or faxed to the appropriate department.
What should I do if I have questions about the form?
If you have questions regarding the ODM 02374 form or the process for submitting it, you can call the Ohio Department of Medicaid at 614-466-6742. They can provide assistance and clarify any uncertainties you may have.
When filling out the Ohio ODM 02374 form, individuals often encounter various pitfalls that can lead to delays or denials in service requests. Here are nine common mistakes to avoid:
Failing to fill out all sections related to the consumer’s information can result in processing delays. Ensure every field is completed, including the consumer's name, address, and Medicaid number.
Providing an incorrect or incomplete Medicaid number can lead to automatic denial of the request. Double-check that the number is accurate and consists of 12 digits.
Not signing the form can halt the entire process. The consumer or authorized representative must provide a signature and date to validate the request.
Submitting requests without confirming the consumer’s Medicaid eligibility can lead to denial. Providers should check eligibility before submitting the form.
Requests for PDN services beyond the standard benefit require additional documentation, such as a physician’s letter. Missing this can result in a denial.
Choosing the wrong waiver type can complicate the request. Ensure that the appropriate waiver (ODA or DODD) is selected based on the consumer's situation.
Independent and agency providers must submit the form through the Medicaid MITS Web Portal. Failing to do so can lead to rejection of the request.
For recertification requests, not providing timely notification for emergency services can result in issues. This notification must be submitted by the next business day.
When requesting changes in services, such as increases or decreases, it’s essential to provide clear justification and supporting documentation. Omitting this can lead to misunderstandings or denials.
By being aware of these common mistakes, individuals can better navigate the process of filling out the Ohio ODM 02374 form and improve their chances of a successful outcome.
The Ohio ODM 02374 form is essential for requesting Private Duty Nursing (PDN) services, but it is often accompanied by several other forms and documents that help streamline the process. Each of these documents serves a specific purpose in ensuring that the request is complete and compliant with state regulations. Below is a list of other commonly used forms and documents that may be needed alongside the ODM 02374.
Each of these documents plays a significant role in the overall process of securing PDN services through Medicaid in Ohio. Ensuring that all forms are completed accurately and submitted in a timely manner can greatly enhance the chances of a successful request. Being thorough and organized can make a positive difference in the experience for both the consumer and the provider.
The Ohio ODM 02374 form is essential for requesting private duty nursing services through Medicaid. It shares similarities with several other important documents used in healthcare and Medicaid services. Here’s a list of nine documents that are comparable to the ODM 02374 form, along with a brief explanation of how they relate:
Understanding these documents can help streamline the process of obtaining necessary services and ensure that all required information is submitted correctly.
When filling out the Ohio ODM 02374 form, it is essential to follow specific guidelines to ensure your request is processed smoothly. Below is a list of things you should and shouldn't do.
Following these guidelines will help ensure that your request for private duty nursing services is processed efficiently and effectively.
Understanding the Ohio ODM 02374 form is crucial for both providers and consumers seeking private duty nursing services. However, several misconceptions can lead to confusion. Here are ten common misunderstandings about this form:
Being aware of these misconceptions can help ensure a smoother experience when navigating the ODM 02374 form. It is essential to approach the process with accurate information and a clear understanding of the requirements.
Eligibility Verification: Before submitting the Ohio ODM 02374 form, ensure the consumer is Medicaid eligible on the date of service. If not, prior authorization requests will be automatically denied.
Complete Consumer Information: Fill out all consumer details accurately, including name, address, Medicaid number, and date of birth. Incomplete forms can lead to delays or denials.
Provider Information Required: The form must include detailed provider information, such as the provider's name, address, and Medicaid provider number. This information is crucial for processing the request.
Emergency Services Notification: If PDN services are provided in an emergency, notify the appropriate authorities by the next business day. Include details about the services and reasons for the emergency.
Submission Guidelines: Submit the form via the Medicaid MITS Web Portal. Do not send faxes or emails for PDN requests, as they will not be accepted.