The Ohio JFS 02390 form plays a crucial role in the home care system, ensuring that individuals receive the necessary support tailored to their health needs. This form is specifically designed for use by Home Care Attendants (HCAs) who are authorized to perform skilled tasks for consumers. It outlines the responsibilities of various parties involved, including the consumer, the authorized health care professional (AHP), the trainer, and the HCA. Each section of the form requires signatures and initials to confirm that the HCA has received proper training for the tasks they will perform. It also emphasizes the importance of communication between the consumer and the HCA, as any changes in health or circumstances must be reported to the appropriate case management agency. The form includes detailed instructions for trainers and health care professionals, ensuring that all parties are aware of their roles in the training and approval process. By documenting the skilled tasks that HCAs are authorized to perform, the JFS 02390 helps maintain a standard of care that is both safe and effective for consumers.

| Fact Name | Details |
|---|---|
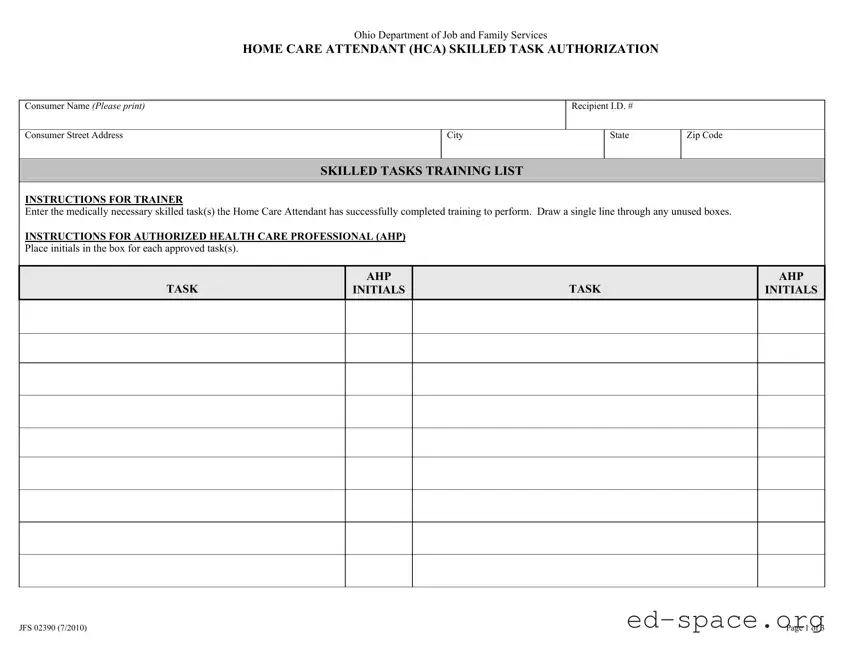
| Form Title | Ohio Department of Job and Family Services Home Care Attendant (HCA) Skilled Task Authorization |
| Form Number | JFS 02390 |
| Effective Date | July 2010 |
| Purpose | This form authorizes a Home Care Attendant to perform medically necessary skilled tasks for a consumer. |
| Consumer Information | Requires the consumer's name, address, and recipient ID number. |
| Training Requirements | Home Care Attendant must complete training for each task listed before performing it. |
| Authorized Health Care Professional | Initials from an authorized health care professional are required for task approval. |
| Revocation of Authorization | Authorization can be revoked at any time by the authorized health care professional. |
| Governing Laws | OAC Rule 5101:3-46-04.1 and OAC Rule 5101:3-50-04.1 govern the use of this form. |
| Duration of Authorization | The effective period for task authorization cannot exceed 12 months. |
Completing the Ohio JFS 02390 form is an essential step in authorizing a Home Care Attendant (HCA) to perform specific skilled tasks. After filling out this form, it will be submitted to the appropriate authorities for processing. The following steps will guide you through the process of accurately completing the form.
What is the Ohio JFS 02390 form?
The Ohio JFS 02390 form is a document used by the Ohio Department of Job and Family Services. It authorizes a Home Care Attendant (HCA) to perform medically necessary skilled tasks for consumers. This form ensures that the HCA has received appropriate training and approval from an Authorized Health Care Professional (AHP).
Who needs to sign the JFS 02390 form?
Several parties must sign the JFS 02390 form. The consumer or their authorized representative must sign to indicate their choice of HCA. The HCA must also sign to confirm their training. Additionally, a trainer and an AHP must sign to validate that the HCA is qualified to perform the specified tasks.
What information is required on the form?
The form requires the consumer's name, address, and recipient ID number. It also includes sections for listing the skilled tasks the HCA has been trained to perform, along with the dates of training and signatures from all involved parties. Accurate completion is crucial for the form's validity.
How long is the authorization valid?
The authorization on the JFS 02390 form is valid for a maximum of 12 months. After this period, the form must be updated to ensure continued compliance with training and approval requirements. It's essential to monitor expiration dates to avoid lapses in authorization.
What happens if the HCA is unable to perform a task?
If the HCA is unable to perform a task due to a change in their ability, they must report this immediately to the consumer, CMA Case Manager, trainer, and AHP. This ensures that appropriate actions can be taken to address the situation and maintain the consumer's care standards.
Can the authorization be revoked?
Yes, the authorization can be revoked at any time by the consumer’s AHP. If the AHP believes that the HCA is no longer suitable for the tasks, they must notify the consumer, CMA Case Manager, and trainer. Revocation protects the consumer's health and safety.
What are the responsibilities of the consumer or authorized representative?
The consumer or authorized representative is responsible for ensuring that the HCA performs tasks according to their training. They must also report any changes in health or circumstances to the Case Management Agency. This oversight is vital for maintaining care quality.
What should be done if there is no physician supporting the HCA option?
If no physician supports the consumer’s decision to use the HCA, the Registered Nurse serving as the AHP must be informed. This communication is critical to ensure that all parties are aware of the situation and can make informed decisions regarding care.
Neglecting to Print Clearly: Many individuals fail to print their information clearly. This can lead to misunderstandings or processing delays. It is crucial to ensure that all names, addresses, and other details are legible.
Missing Required Signatures: One common mistake is not obtaining all necessary signatures. Each party involved, including the consumer, home care attendant, trainer, and authorized health care professional, must sign the form. Omitting any signature can render the form invalid.
Incorrectly Initialing Approved Tasks: The authorized health care professional must initial each task that the home care attendant is approved to perform. Failing to initial all applicable tasks can result in delays or denials of approval.
Forgetting to Update Changes: Changes in health status or circumstances must be reported to the case management agency. Not doing so can lead to complications in care and potential liability issues.
Omitting Training Details: It is essential to provide a detailed description of how the home care attendant will perform each task. This includes specifying times or intervals. Lack of detail can lead to confusion and improper care.
Failing to Review Instructions: Some individuals skip reading the instructions provided on the form. Understanding the requirements for each section is critical to ensure compliance and proper authorization.
Ignoring the Effective Period: The form must specify an effective period for the tasks authorized, which should not exceed 12 months. Neglecting to include this information can result in the form being deemed incomplete.
The Ohio JFS 02390 form is an important document used in the home care industry. It authorizes a Home Care Attendant (HCA) to perform specific skilled tasks for a consumer. Along with this form, several other documents are often required to ensure proper care and compliance. Below is a list of related forms and documents that may be used alongside the JFS 02390.
These documents work together to create a comprehensive framework for home care services. They ensure that both the consumer and the Home Care Attendant are protected and that quality care is delivered. Proper documentation is key to maintaining standards and providing effective support.
The Ohio JFS 02390 form is essential for authorizing skilled tasks for Home Care Attendants (HCA). Several other documents serve similar purposes in different contexts. Here are six documents that share similarities with the JFS 02390 form:
When filling out the Ohio JFS 02390 form, it is essential to ensure accuracy and clarity. Here are some important do's and don'ts to keep in mind:
Understanding the Ohio JFS 02390 form is essential for consumers, home care attendants, and healthcare professionals. However, several misconceptions can lead to confusion. Here are five common misunderstandings:
By clarifying these misconceptions, individuals can better navigate the use of the Ohio JFS 02390 form and ensure that care is delivered effectively and safely.
When filling out and using the Ohio JFS 02390 form, it's important to understand the key aspects of the process. Here are some essential takeaways:
By following these guidelines, you can ensure that the Ohio JFS 02390 form is filled out correctly and used effectively. This will help maintain compliance and ensure the best care for the consumer.