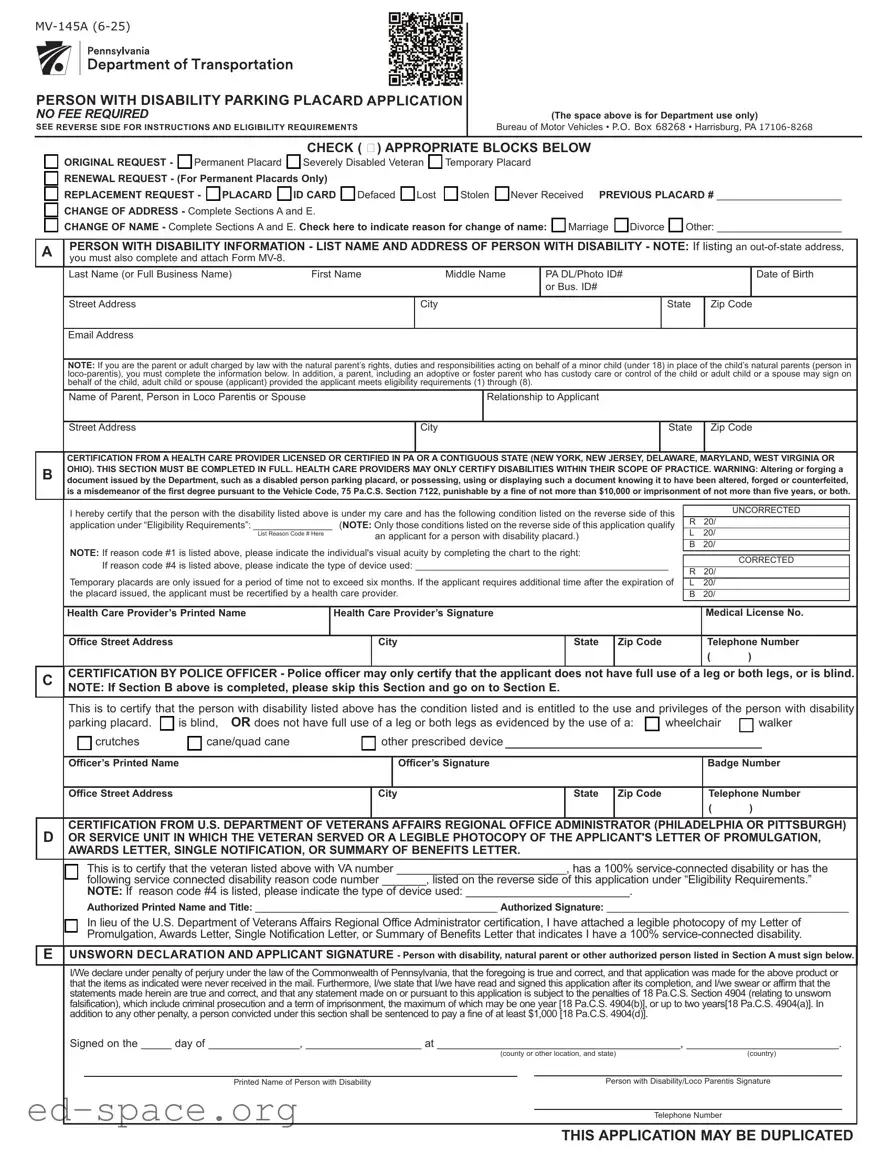
The MV-145A form serves as a critical tool for individuals seeking a parking placard designated for persons with disabilities in Pennsylvania. This application is designed to streamline the process for obtaining various types of placards, including permanent, temporary, and those specifically for severely disabled veterans. Importantly, there is no fee associated with this application, making it accessible to those in need. The form requires applicants to provide personal information, including their name, address, and details about their disability. A health care provider must also certify the disability, ensuring that only eligible individuals receive the benefits associated with the placard. The MV-145A includes sections for renewals, replacements, and changes of address or name, allowing for flexibility as circumstances change. Additionally, it outlines the eligibility requirements, ensuring that applicants understand the criteria necessary to qualify for a placard. With clear instructions provided on the reverse side, this form aims to simplify the application process while maintaining the integrity of the program designed to assist those with disabilities.
PERSON WITH DISABILITY PARKING PLACARD APPLICATION NO FEE REQUIRED SEE REVERSE SIDE FOR INSTRUCTIONS AND ELIGIBILITY REQUIREMENTS
(The space above is for Department use only)
Bureau of Motor Vehicles • P.O. Box 68268 • Harrisburg, PA
CHECK ( 4) APPROPRIATE BLOCKS BELOW
qORIGINAL REQUEST - q Permanent Placard q Severely Disabled Veteran q Temporary Placard
qRENEWAL REQUEST - (For Permanent Placards Only)
q REPLACEMENT REQUEST - q PLACARD q ID CARD q Defaced q Lost q Stolen q Never Received PREVIOUS PLACARD # ______________________
qCHANGE OF ADDRESS - Complete Sections A and E.
qCHANGE OF NAME - Complete Sections A and E. Check here to indicate reason for change of name: q Marriage q Divorce q Other: ______________________
APERSON WITH DISABILITY INFORMATION - LIST NAME AND ADDRESS OF PERSON WITH DISABILITY - NOTE: If listing an
|
Last Name (or Full Business Name) |
First Name |
|
|
|
Middle Name |
PA DL/Photo ID# |
|
|
|
Date of Birth |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
or Bus. ID# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Street Address |
|
|
|
|
|
|
|
City |
|
|
|
State |
Zip Code |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Email Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
NOTE: If you are the parent or adult charged by law with the natural parent’s rights, duties and responsibilities acting on behalf of a minor child (under 18) in place of the child’s natural parents (person in |
||||||||||||||||||||||
|
|||||||||||||||||||||||
|
behalf of the child, adult child or spouse (applicant) provided the applicant meets eligibility requirements (1) through (8). |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Name of Parent, Person in Loco Parentis or Spouse |
|
|
|
|
|
|
|
Relationship to Applicant |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Street Address |
|
|
|
|
|
|
|
City |
|
|
|
State |
Zip Code |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
CERTIFICATION FROM A HEALTH CARE PROVIDER LICENSED OR CERTIFIED IN PA OR A CONTIGUOUS STATE (NEW YORK, NEW JERSEY, DELAWARE, MARYLAND, WEST VIRGINIA OR |
||||||||||||||||||||||
B |
OHIO). THIS SECTION MUST BE COMPLETED IN FULL. HEALTH CARE PROVIDERS MAY ONLY CERTIFY DISABILITIES WITHIN THEIR SCOPE OF PRACTICE. WARNING: Altering or forging a |
||||||||||||||||||||||
document issued by the Department, such as a disabled person parking placard, or possessing, using or displaying such a document knowing it to have been altered, forged or counterfeited, |
|||||||||||||||||||||||
|
is a misdemeanor of the first degree pursuant to the Vehicle Code, 75 Pa.C.S. Section 7122, punishable by a fine of not more than $10,000 or imprisonment of not more than five years, or both. |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
I hereby certify that the person with the disability listed above is under my care and has the following condition listed on the reverse side of this |
|
|
UNCORRECTED |
|||||||||||||||||||
|
application under “Eligibility Requirements”: _______________ |
(NOTE: Only those conditions listed on the reverse side of this application qualify |
R |
20/ |
|
|
|
|
|
||||||||||||||
|
|
|
List Reason Code # Here |
|
|
an applicant for a person with disability placard.) |
|
|
L |
20/ |
|
|
|
|
|
||||||||
|
NOTE: If reason code #1 is listed above, please indicate the individual's visual acuity by completing the chart to the right: |
|
|
B |
20/ |
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
If reason code #4 is listed above, please indicate the type of device used: ________________________________________________ |
|
|
CORRECTED |
|
|||||||||||||||||
|
|
R |
20/ |
|
|
|
|
|
|||||||||||||||
|
Temporary placards are only issued for a period of time not to exceed six months. If the applicant requires additional time after the expiration of |
|
|
|
|
|
|||||||||||||||||
|
L |
20/ |
|
|
|
|
|
||||||||||||||||
|
the placard issued, the applicant must be recertified by a health care provider. |
|
|
|
|
B |
20/ |
|
|
|
|
|
|||||||||||
|
Health Care Provider’s Printed Name |
|
|
Health Care Provider’s Signature |
|
|
|
|
|
Medical License No. |
|||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Office Street Address |
|
|
|
|
City |
|
State |
Zip Code |
|
Telephone Number |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
C |
CERTIFICATION BY POLICE OFFICER - Police officer may only certify that the applicant does not have full use of a leg or both legs, or is blind. |
||||||||||||||||||||||
|
NOTE: If Section B above is completed, please skip this Section and go on to Section E. |
|
|
|
|
|
|
|
|
|
|||||||||||||
|
This is to certify that the person with disability listed above has the condition listed and is entitled to the use and privileges of the person with disability |
||||||||||||||||||||||
|
parking placard. |
q is blind, OR does not have full use of a leg or both legs as evidenced by the use of a: q wheelchair |
q walker |
||||||||||||||||||||
|
|
q crutches |
q cane/quad cane |
|
|
|
q other prescribed device |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Officer’s Printed Name |
|
|
|
|
|
Officer’s Signature |
|
|
|
|
|
Badge Number |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Office Street Address |
|
|
|
|
City |
|
State |
Zip Code |
|
Telephone Number |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
D |
CERTIFICATION FROM U.S. DEPARTMENT OF VETERANS AFFAIRS REGIONAL OFFICE ADMINISTRATOR (PHILADELPHIA OR PITTSBURGH) |
||||||||||||||||||||||
OR SERVICE UNIT IN WHICH THE VETERAN SERVED OR A LEGIBLE PHOTOCOPY OF THE APPLICANT'S LETTER OF PROMULGATION, |
|||||||||||||||||||||||
|
AWARDS LETTER, SINGLE NOTIFICATION, OR SUMMARY OF BENEFITS LETTER. |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
q |
This is to certify that the veteran listed above with VA number ___________________________, has a 100% |
|||||||||||||||||||||
|
|
following service connected disability reason code number _______, listed on the reverse side of this application under “Eligibility Requirements.” |
|||||||||||||||||||||
|
|
NOTE: If reason code #4 is listed, please indicate the type of device used: __________________________. |
|
|
|
|
|
|
|
||||||||||||||
|
|
Authorized Printed Name and Title: ____________________________________________ Authorized Signature: ____________________________________________ |
|||||||||||||||||||||
|
q |
In lieu of the U.S. Department of Veterans Affairs Regional Office Administrator certification, I have attached a legible photocopy of my Letter of |
|||||||||||||||||||||
|
|
Promulgation, Awards Letter, Single Notification Letter, or Summary of Benefits Letter that indicates I have a 100% |
|||||||||||||||||||||
E |
UNSWORN DECLARATION AND APPLICANT SIGNATURE - Person with disability, natural parent or other authorized person listed in Section A must sign below. |
|
|||||||||||||||||||||
I/We declare under penalty of perjury under the law of the Commonwealth of Pennsylvania, that the foregoing is true and correct, and that application was made for the above product or that the items as indicated were never received in the mail. Furthermore, I/we state that I/we have read and signed this application after its completion, and I/we swear or affirm that the statements made herein are true and correct, and that any statement made on or pursuant to this application is subject to the penalties of 18 Pa.C.S. Section 4904 (relating to unsworn falsification), which include criminal prosecution and a term of imprisonment, the maximum of which may be one year [18 Pa.C.S. 4904(b)], or up to two years[18 Pa.C.S. 4904(a)]. In addition to any other penalty, a person convicted under this section shall be sentenced to pay a fine of at least $1,000 [18 Pa.C.S. 4904(d)].
Signed on the _____ day of _______________, ___________________ at ________________________________________, _________________________.
|
(county or other location, and state) |
(country) |
||
|
|
|
|
|
Printed Name of Person with Disability |
|
|
Person with Disability/Loco Parentis Signature |
|
|
|
|
|
|
|
|
|
|
Telephone Number |
THIS APPLICATION MAY BE DUPLICATED
INSTRUCTIONS
1.Permanent Placard - Complete Sections A, B or C (NOT BOTH) and E. NOTE: Individuals should list their PA Driver’s License (PA DL) or Photo ID# in the space provided. Businesses should list their Business ID# (Bus. ID) where indicated (i.e. E.I.N.).
2.Severely Disabled Veteran Placard - Complete Sections A, D and E.
3.Temporary Placard - Complete Sections A, B and E. NOTE: Only licensed health care providers* may certify disabilities for temporary placards. Temporary placards may be issued for a period up to six months and may not be extended for an additional period of time. When additional time is needed, a new application must be completed and certified by a health care provider. In addition, please list your previous placard number.
4.Renewal Request - Complete Sections A and E.
5.Replacement Request - Indicate if applying for a replacement placard or ID card. Please check reason for replacement; Lost, Stolen, Defaced or Never Received. List your previous placard number and complete Sections A and E. NOTE: If product was not received within 90 days, please check the "Never Received" box or if product was not received for over 90 days please check the "Lost" box.
6.Change of Address - Complete Sections A and E.
7.Change of Name - Complete Sections A and E. Check the block on the front of this application to indicate reason for change of name.
*Health Care Provider is defined as a physician, chiropractor, optometrist, podiatrist, physician assistant, or a certified registered nurse practitioner licensed or certified in Pennsylvania or a contiguous state. Health care providers may only certify disabilities within their scope of practice.
NOTE: Customers with a permanent placard have the option to renew their placard, request a replacement placard or change the address their placard online at https://www.placard.penndot.pa.gov/PlacardWeb/public/external/placardLogin.xhtml or scan the QR code on the front of this application.
Placard Type |
Eligibility Requirements |
Qualifying Vehicles |
Benefits |
Person with Disability Placard
“Reason Codes”
Applicant:
(1)is blind.
(2)does not have full use of an arm or both arms.
(3)cannot walk 200 feet without stopping to rest.
(4)cannot walk without the use of, or assistance from, a brace, cane, crutch, another person, prosthetic device, wheelchair or other assistive device.
(5)is restricted by lung disease to such an extent that the person’s forced (respiratory) expiratory volume for one second, when measured by spirometry, is less than one liter or the arterial oxygen tension is less than 60 MM/HG on room air at rest.
(6)uses portable oxygen.
(7)has a cardiac condition to the extent that the person’s functional limitations are classified in severity as Class III or Class IV according to the standards set by the American Heart Association.
(8)is severely limited in their ability to walk due to an arthritic, neurological or orthopedic condition.
NOTE: If you are the parent or adult charged by law with the natural parent’s rights, duties, and responsibilities, acting on behalf of a minor child (under 18) in place of the child’s natural parents (person in
In addition, a parent, including an adoptive or foster parent who has custody, care, or control of the child or adult child or a spouse, may sign on behalf of the child, adult child, or spouse (applicant) provided the person with disability meets eligibility requirements (1) through (8).
(1)The placard is required to be displayed when the vehicle is parked in areas designated for use by persons with disability only and must not be displayed when the vehicle is being operated on the highway.
NOTE: Organizations that operate a passenger vehicle to transport persons with disabilities must supply the Department with the following:
a)A notarized statement of how the placard will be used and the type of services that will be provided.
b)The weekly or monthly number of hours that the services are provided.
c)The make of the vehicle(s), including the title number, vehicle identification number and registration plate number. The vehicle(s) must be titled in the name of the organization and must be a passenger vehicle.
d)The number of placards required: (Organizations may not be issued more than eight placards in the organization’s name.)
(1)Parking permitted in spaces designated for disabled persons and for 60 minutes in excess of legal parking period except where local ordinances or police regulations provide for the accommodation
of heavy traffic during morning, afternoon or evening hours.
(2)Upon request of a person with disability, local authorities may erect on the highway as close as possible to the person’s residence a sign(s) indicating that the place is reserved for the person with disability, that no one else may park there unless a person with disability plate or placard is displayed and that any unauthorized person parking there will be subject to a fine.
Severely
Disabled
Veteran
Placard
(1)100%
(2)Same disabilities as listed above for Person with Disability Placard but must be
Same as 1 and 2 above for Person with Disability Placard.
Same as above for Person with Disability Placard.
Use of Person with Disability and Severely Disabled Veteran Placards:
. Parking in a designated persons with disability parking space is only permitted with this parking placard when the vehicle is being used for the transportation of the person for which the parking placard was issued.
. Any vehicle lawfully displaying a parking placard will qualify for parking in areas designated only for use by persons with a disability. NOTE: This parking placard can not be used to park where parking is prohibited.
Send completed application to: PennDOT, Bureau of Motor Vehicles, P.O. Box 68268, Harrisburg, PA
Visit us at www.pa.gov/dmv or call us at
| Fact Name | Details |
|---|---|
| Purpose | The MV-145A form is used to apply for a Person with Disability Parking Placard in Pennsylvania. |
| No Fee Required | There is no fee associated with submitting the MV-145A application. |
| Eligibility Requirements | Applicants must meet specific disability criteria outlined on the form, such as being blind or having limited mobility. |
| Governing Law | The form is governed by Pennsylvania's Vehicle Code, specifically 75 Pa.C.S. Section 7122. |
Completing the MV-145A form is essential for obtaining a person with disability parking placard. This process requires careful attention to detail to ensure all information is accurately provided. Following the steps below will help you navigate through the application efficiently.
After submitting the application, you will await processing by the Bureau of Motor Vehicles. Keep an eye on your mail for any updates or requests for additional information. It is crucial to ensure that all details are correct to avoid delays in receiving your placard.
What is the MV-145A form used for?
The MV-145A form is an application for a Person with Disability Parking Placard in Pennsylvania. It allows individuals with disabilities to apply for a parking placard that provides access to designated parking spaces. This form can be used for original requests, renewals, replacements, and changes of address or name. Importantly, there is no fee required to submit this application.
Who is eligible to apply for a disability parking placard?
Eligibility for a disability parking placard is determined by specific medical conditions. The applicant must meet one of the criteria listed on the form, such as being blind, having limited use of limbs, or being unable to walk a certain distance without resting. Additionally, the application can be completed by a parent or guardian acting on behalf of a minor child, provided they meet the eligibility requirements.
What information is required to complete the MV-145A form?
To complete the MV-145A form, applicants need to provide personal information, including their name, address, date of birth, and Pennsylvania driver's license or photo ID number. If the applicant is a minor, the form must also include details about the parent or guardian. A health care provider must certify the disability, and their information must be included as well. If applicable, the applicant should indicate any changes in name or address and provide the previous placard number for renewals or replacements.
How long is a temporary disability parking placard valid?
A temporary disability parking placard is valid for a maximum of six months. If the applicant requires additional time beyond this period, they must submit a new application and obtain recertification from a licensed health care provider. It is essential to note that temporary placards cannot be extended; a new application is necessary for continued use.
What should I do if my placard is lost or stolen?
If a disability parking placard is lost, stolen, or defaced, the applicant must complete the MV-145A form to request a replacement. The applicant should indicate the reason for the replacement and provide their previous placard number if applicable. This application should be sent to the Bureau of Motor Vehicles in Harrisburg, PA, and no notarization is required for this request.
Incorrectly selecting the type of placard. Individuals often fail to check the appropriate box for the type of placard they are requesting, such as Permanent, Temporary, or Severely Disabled Veteran. This can lead to delays in processing their application.
Omitting required personal information. Applicants sometimes forget to include essential details, such as their full name, address, and date of birth. Missing this information can result in the application being returned or rejected.
Failing to provide a valid health care provider certification. The certification section must be completed by a licensed health care provider. Incomplete or incorrect certifications can lead to disqualification.
Neglecting to sign the application. It is crucial for the applicant or authorized person to sign the application. An unsigned application is considered incomplete and will not be processed.
Not including the previous placard number when applicable. When applying for a renewal or replacement, applicants often forget to include their previous placard number, which is necessary for processing the request.
Ignoring the instructions for notarization. While notarization is not required for most applications, some applicants mistakenly believe it is necessary and delay their submission as a result.
The MV-145A form is essential for individuals seeking a parking placard for persons with disabilities. However, several other forms and documents are often used in conjunction with it. Each of these documents serves a specific purpose, ensuring that applicants can navigate the process smoothly and efficiently.
Understanding these accompanying documents can greatly assist individuals in successfully applying for and maintaining their disability parking placards. Each form plays a vital role in the overall process, ensuring that applicants receive the support and accommodations they need.
When filling out the MV-145A form, it is important to be careful and thorough. Here are some guidelines to help you:
Following these guidelines will help ensure that your application is processed smoothly. If you have any questions, don't hesitate to reach out for assistance.
Understanding the MV-145A form is essential for individuals seeking a disability parking placard in Pennsylvania. However, several misconceptions can lead to confusion. Here are nine common misconceptions about the MV-145A form:
Addressing these misconceptions can streamline the application process and ensure that individuals receive the appropriate placards in a timely manner.
Here are some important points to keep in mind when filling out and using the MV 145A form for a Person with Disability Parking Placard:
Following these guidelines will help ensure a smooth application process and proper use of your disability parking placard.