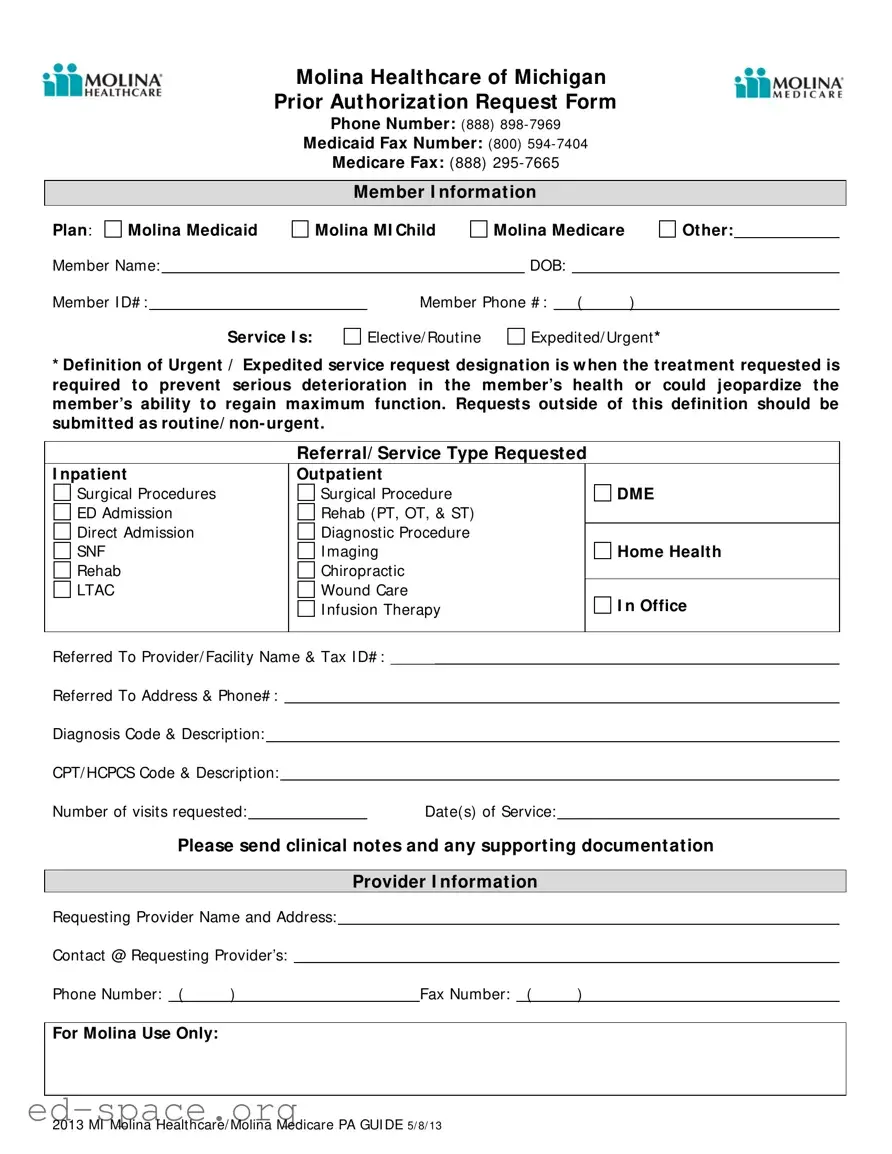
The Michigan Molina Prior Authorization form serves as a critical tool for healthcare providers seeking approval for various medical services on behalf of their patients. This form is essential for ensuring that services are covered under Molina Healthcare's Medicaid and Medicare plans. It includes key sections such as member information, service type, and provider details, which must be filled out accurately to facilitate the authorization process. Members can indicate whether the service is elective or urgent, with urgent requests defined as those necessary to prevent serious health deterioration. The form also requires specific information about the requested services, including diagnosis codes and CPT/HCPCS codes, to ensure proper categorization and approval. Additionally, providers must submit clinical notes and any supporting documentation to substantiate the request. With dedicated contact numbers for inquiries and fax submissions, the form aims to streamline communication between healthcare providers and Molina Healthcare, ultimately enhancing patient care and access to necessary treatments.
Molina Healthcare of Michigan Prior Authorization Request Form
Phone Number: (888)
Medicaid Fax Number: (800)
Medicare Fax: (888)
Member I nformat ion
Plan: |
Molina Medicaid |
Member Name:
Molina MI Child
Molina Medicare
DOB:
Other:
Member I D# : |
|
Member Phone # : |
( |
) |
Service I s:
Elective/ Routine
Expedited/ Urgent *
*Definition of Urgent / Expedited service request designation is w hen the treat ment requested is required to prevent serious deterioration in the member’s health or could jeopardize the member’s ability to regain maximum function. Requests outside of this definition should be submitted as routine/ non- urgent.
Referral/ Service Type Request ed
|
I npatient |
|
|
|
|
|
|
Outpatient |
|
|
|
||||||
|
Surgical Procedures |
|
|
|
|
|
|
Surgical Procedure |
|
DME |
|
||||||
|
ED Admission |
|
|
|
|
|
|
Rehab (PT, OT, & ST) |
|
|
|
||||||
|
Direct Admission |
|
|
|
|
|
|
Diagnostic Procedure |
|
|
|
||||||
|
SNF |
|
|
|
|
|
|
I maging |
|
Home Health |
|
||||||
|
Rehab |
|
|
|
|
|
|
Chiropractic |
|
|
|
||||||
|
LTAC |
|
|
|
|
|
|
Wound Care |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
I nfusion Therapy |
|
I n Office |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Referred To Provider/ Facility Name & Tax I D# : _____ |
|
|
|
|||||||||||||
|
Referred To Address & Phone# : |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Diagnosis Code & Description: |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
CPT/ HCPCS Code & Description: |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Number of visits requested: |
|
|
|
|
|
Date(s) of Service: |
|
|
|
|||||||
|
|
Please send clinical not es and any support ing document at ion |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Provider I nformat ion |
|
|
|
||||
|
Requesting Provider Name and Address: |
|
|
|
|||||||||||||
|
Contact @ Requesting Provider’s: |
|
|
|
|
|
|
|
|
|
|
||||||
|
Phone Number: ( |
) |
|
|
|
|
|
|
|
|
Fax Number: ( |
) |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
For Molina Use Only: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2013 MI Molina Healthcare/ Molina Medicare PA GUI DE 5/ 8/ 13
| Fact Name | Details |
|---|---|
| Form Purpose | The Michigan Molina Prior Authorization form is used to request approval for medical services. |
| Contact Information | For inquiries, call Molina Healthcare at (888) 898-7969. |
| Medicaid Fax Number | Send Medicaid requests to (800) 594-7404. |
| Medicare Fax Number | Medicare requests should be faxed to (888) 295-7665. |
| Member Information | Include the member's name, ID number, and date of birth on the form. |
| Service Types | Requests can be for inpatient, outpatient, surgical procedures, and more. |
| Urgent Requests | Urgent requests are for services needed to prevent serious health deterioration. |
| Documentation Required | Clinical notes and supporting documents must accompany the request. |
| Provider Information | Provide the requesting provider's name, address, and contact details. |
| Governing Laws | This form is governed by Michigan Medicaid and Medicare regulations. |
Filling out the Michigan Molina Prior Authorization form is a straightforward process. Once you have completed the form, you can submit it to the appropriate fax number based on the member's plan. Ensure you have all the necessary information ready to avoid delays in processing your request.
Once the form is filled out completely, review it for accuracy. Then, fax it to the appropriate number: (800) 594-7404 for Medicaid or (888) 295-7665 for Medicare. Keep a copy for your records.
What is the purpose of the Michigan Molina Prior Authorization form?
The Michigan Molina Prior Authorization form is used to request approval for specific medical services before they are provided. This process ensures that the requested services are medically necessary and covered under the member's plan. It helps streamline care and ensures that members receive appropriate treatments in a timely manner.
How do I submit the Prior Authorization request?
You can submit the Prior Authorization request by completing the form and sending it via fax. For Medicaid requests, use the fax number (800) 594-7404. For Medicare requests, send it to (888) 295-7665. Ensure that you include all required information, including diagnosis codes and supporting documentation, to avoid delays in processing.
What types of services require Prior Authorization?
Prior Authorization is typically required for various services such as inpatient and outpatient procedures, surgical procedures, diagnostic tests, and certain therapies like physical or occupational therapy. It is crucial to determine whether the service is elective/routine or urgent/expedited. Urgent requests must meet specific criteria to be considered for expedited review.
What information do I need to provide on the form?
When filling out the form, you must provide detailed information, including the member's name, ID number, date of birth, and contact information. Additionally, specify the type of service requested, diagnosis codes, CPT/HCPCS codes, and the number of visits needed. Don't forget to include clinical notes and any other supporting documentation to ensure a smooth approval process.
Incomplete Member Information: Failing to fill out all required member details, such as the Member ID number or date of birth, can lead to delays in processing the request.
Incorrect Service Type Selection: Choosing the wrong service type, like elective instead of urgent, can result in the request being denied or delayed.
Missing Diagnosis and CPT Codes: Not providing the correct diagnosis code and CPT/HCPCS code can hinder the approval process. These codes are essential for understanding the medical necessity of the request.
Omitting Clinical Notes: Not including clinical notes or supporting documentation can cause the request to be flagged for further review, prolonging the approval time.
Incorrect Provider Information: Listing an incorrect provider name or contact information can lead to confusion and miscommunication, delaying the authorization process.
Failure to Specify Number of Visits: Not indicating the number of visits requested can lead to assumptions that may not align with the actual treatment plan, affecting the approval.
Ignoring Submission Guidelines: Not following the specified submission guidelines, such as using the correct fax number, can result in the request not being received or processed.
When submitting the Michigan Molina Prior Authorization form, several other documents may be needed to ensure a smooth process. These documents help provide the necessary information for the authorization request and support the medical necessity of the services requested. Below is a list of commonly used forms and documents that may accompany the prior authorization request.
Having these documents ready can significantly streamline the authorization process. It ensures that all necessary information is provided, which can lead to a quicker decision from Molina Healthcare. Always check with the specific requirements for your situation to ensure compliance and avoid delays.
The Michigan Molina Prior Authorization form serves as a critical document in the healthcare process, particularly for Medicaid and Medicare services. Its structure and purpose share similarities with several other documents used in healthcare settings. Below is a list of ten such documents, highlighting their similarities with the Molina form.
When filling out the Michigan Molina Prior Authorization form, it's essential to follow specific guidelines to ensure a smooth process. Here’s a list of what to do and what to avoid:
By adhering to these guidelines, you can help facilitate a more efficient authorization process for the services needed.
Below is a list of common misconceptions regarding the Michigan Molina Prior Authorization form, along with clarifications for each:
This is incorrect. The form is applicable to both Medicaid and Medicare members. It is essential for all members to complete the form accurately, regardless of their plan.
While urgent services may require expedited processing, they still need prior authorization. The definition of urgent services is specific and must be adhered to.
Approval is not guaranteed. The request will be reviewed based on medical necessity and compliance with Molina’s guidelines.
While physicians typically submit the form, other authorized providers can also complete and submit it on behalf of the member.
Different services may require varying levels of documentation. It is important to include all relevant clinical notes and supporting documents as specified for the service type requested.
A diagnosis code is necessary for the review process. Omitting this information can lead to delays or denial of the authorization request.
Timely submission is critical. Requests should be submitted as soon as possible to avoid delays in treatment.
While faxing is one method, providers may have other options for submission. It is advisable to check with Molina for all available submission methods.
When filling out and using the Michigan Molina Prior Authorization form, it is essential to keep several key points in mind to ensure a smooth process. The following takeaways provide guidance on how to effectively complete and utilize the form:
By adhering to these guidelines, individuals can facilitate a more efficient prior authorization process with Molina Healthcare of Michigan. This careful attention to detail can significantly impact the member's access to necessary healthcare services.