In today's multifaceted healthcare landscape, diligent record-keeping stands out as an indispensable component, ensuring the safe and accurate administration of medications to individuals in various settings. The Medication Administration Record Sheet serves as a vital tool in this rigorous process, meticulously documenting every aspect of drug dispensation - from the patient’s name and the attending physician's details to the precise timings across the month for administering medications. Each entry on the form not only marks the time and date for each dose but also accounts for any changes in medication, doses missed for reasons such as refusal by the consumer or discontinuation on a physician's advice, and notations for when the individual is at home or participating in day programs. This comprehensive approach facilitates healthcare providers in maintaining a clear and current overview of an individual's medication regimen, thereby playing a critical role in safeguarding against the risks of errors in medication administration and ensuring optimal care outcomes. By summarizing the complex interplay of factors represented within the Medication Administration Record Sheet, one gains insight into its fundamental importance in the broader context of health and wellness management.
| Fact Number | Detail |
|---|---|
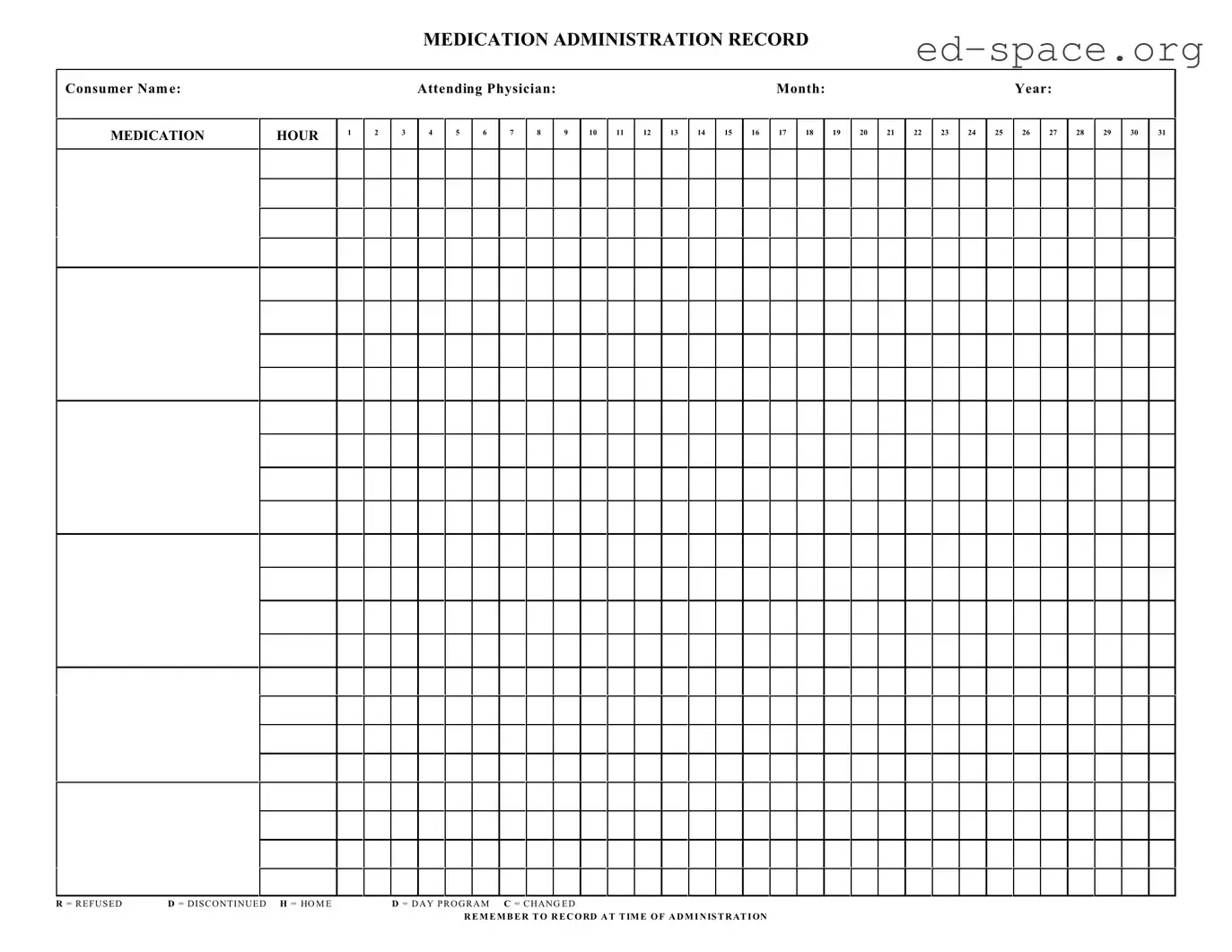
| 1 | The Medication Administration Record Sheet is a tool used to document all medications administered to a consumer, ensuring accuracy and safety. |
| 2 | It includes sections for the consumer's name, attending physician, medication hour, and columns for each day of the month to record administration details. |
| 3 | Codes such as "R" for refused, "D" for discontinued, "H" for home, "D" for day program, and "C" for changed help in quickly documenting the status of each medication dose. |
| 4 | The form prompts caregivers to remember to record at the time of administration, ensuring timely and accurate entries. |
| 5 | Medication Administration Record Sheets are crucial for compliance with state laws and regulations governing medication administration in healthcare settings. |
| 6 | In some states, the form is standardized, and its use is mandated by specific health department regulations to maintain consistency and reliability across care settings. |
| 7 | Proper use of the form can help in legal and regulatory compliance, providing documentation that medication was administered as prescribed. |
| 8 | Reviewing completed forms can offer insights into a consumer's medication management over time, facilitating better healthcare outcomes. |
| 9 | It serves as a communication tool between caregivers and healthcare professionals, ensuring continuity and coordination of care. |
| 10 | Digital versions of the Medication Administration Record Sheet allow for easier storage, retrieval, and sharing of data while still being governed by privacy and security regulations. |
Filling out the Medication Administration Record (MAR) Sheet properly is crucial to ensure accurate tracking of medications for individuals under care. This form plays an essential role in healthcare settings, documenting when and what medications have been administered. Below is a guide on how to complete this form, step by step. Remember, accuracy is key to safeguarding the health and well-being of those you're supporting.
After completing the form, review it for accuracy. Accurate medication management is crucial for the health and safety of those in care. Therefore, take the time to ensure that every detail on the Medication Administration Record Sheet is correctly filled out and up to date.
What is a Medication Administration Record Sheet?
A Medication Administration Record Sheet is a document used to track the administration of medications to an individual over a specific period of time. This sheet records essential details such as the name of the person receiving medication, the type of medication, dosage, the time medication is taken, and any notes related to changes in medication, refusal of medication, or medication taken while away from home or in a day program.
Who needs to use a Medication Administration Record Sheet?
This form is typically used by caregivers, healthcare professionals, and facilities that provide care to individuals requiring assistance with medication management. It is especially useful in settings where multiple individuals are responsible for administering medications, such as in senior care facilities, hospitals, or in home care scenarios.
Why is it important to record medication administration?
Recording medication administration is crucial for ensuring the safety and well-being of the individual receiving care. It helps in monitoring dosage accuracy, timing of medication, and identifying any side effects or adverse reactions. This record also facilitates communication among caregivers and healthcare professionals, making it easier to track the effectiveness of medications and make necessary adjustments.
How should the Medication Administration Record Sheet be filled out?
When filling out the sheet, it's important to write legibly and include all relevant details such as the consumer's name, the medication name, the dosage, and the specific time of administration. Any changes in medication, instances where medication is refused, or when medication is taken while away from the usual care setting should be clearly noted using the designated symbols (R for refused, D for discontinued, H for home, D for day program, C for changed).
Can this sheet be used for multiple months?
No, the Medication Administration Record Sheet is designed for use over a single month. Each month requires a new form to ensure accurate and up-to-date recording of medication administration. This monthly approach helps in effective monitoring and management of the individual's medication regimen.
What should be done if a medication is refused or discontinued?
Any instances where medication is refused by the individual or discontinued by the attending physician should be immediately recorded on the sheet using the appropriate symbol (R for refused, D for discontinued). Additional notes detailing the reason for refusal or discontinuation and the date of occurrence should also be included. This information is critical for healthcare providers to review and take necessary actions.
How is medication administered outside of the home or in a day program documented?
Medication administered outside of the usual care setting, such as in a day program or while the individual is at home (and not under the direct care of the facility or caregiver), should be documented using the symbols H for home and D for day program. It is important to also record the time of administration and any other relevant details to ensure continuity in the medication management process.
What does the letter C stand for in the medication administration process?
The letter C stands for "Changed" on the Medication Administration Record Sheet. It is used to indicate any changes to the medication regimen, including changes in dosage, frequency, or the medication itself. Detailing these changes on the sheet ensures accurate tracking and helps in assessing the effectiveness of the medication regimen over time.
Is it necessary to record the time of medication administration?
Yes, recording the exact time of medication administration is essential. It ensures that medications are given at the correct intervals, avoids missed or duplicate doses, and helps in monitoring the medication's effectiveness and any potential side effects. This practice is crucial for maintaining the individual's health and safety.
Who should have access to the Medication Administration Record Sheet?
Access to the Medication Administration Record Sheet should be limited to individuals directly involved in the care and medication management of the consumer, such as healthcare professionals, caregivers, and authorized facility staff. It's important to keep this information confidential and secure to protect the privacy and well-being of the individual receiving care.
When filling out the Medication Administration Record Sheet, there are several common mistakes that can be avoided to ensure accurate and effective documentation. These errors not only risk the health and safety of the consumers but can also lead to miscommunications between healthcare providers. Here is a closer look at these common errors:
Not updating the consumer's name and month/year at the top of the form can lead to confusion, especially when managing records for multiple individuals or across different time periods.
Omitting the attending physician's name can result in uncertainties, especially if there are questions about the prescribed medications or if a consultation is necessary.
Failure to mark the correct medication hour precisely can complicate the administration schedule, potentially leading to missed or double dosages.
Overlooking the special codes like R for refused, D for discontinued, H for home, and C for changed, compromises the accuracy of the record, hindering proper medication tracking and adjustments.
Not recording administrations at the time they are given can result in unreliable documentation, reducing the effectiveness of the medication regimen and possibly endangering the consumer's health.
Misunderstanding the codes used on the form can lead to incorrect entries, such as marking a medication as discontinued when it was merely refused at a specific administration time.
Forgetting to review and update the form for any medication changes throughout the month can result in administering outdated prescriptions.
Lastly, neglecting to provide a signature or initials next to each entry leaves the record unverified, which can question the credibility and accuracy of the medication administration activities documented.
Avoiding these mistakes ensures the Medication Administration Record Sheet serves its purpose effectively, maintaining the safety and well-being of consumers under care. It's crucial for healthcare providers to pay careful attention to detail and regularly update these records to reflect current and accurate medication management.
When caring for individuals, especially in healthcare or caregiving settings, a Medication Administration Record (MAR) sheet is a pivotal document. However, to provide comprehensive care, various other forms and documents typically accompany the MAR sheet. These documents ensure that the individual receives not only proper medication but also holistic care tailored to their specific needs. Here are some of the key documents often used alongside the Medication Administration Record Sheet.
Together with the Medication Administration Record Sheet, these documents form a comprehensive toolkit for ensuring safe and effective care. They support the delivery of care that respects each individual's unique needs, promotes their well-being, and guards against potential medication errors. By integrating these forms into the care process, healthcare providers can offer a more detailed, person-centered approach to medication management and overall care.
Daily Activity Log: Similar to the Medication Administration Record Sheet, the Daily Activity Log tracks activities over a period, typically a month, marking the time and nature of each activity. Both documents serve as a precise record of events or actions taken within specific time slots throughout the day, making it easier to review patterns or ensure consistency and accountability.
Patient Care Report: This document is used by emergency medical services (EMS) to detail the care given to a patient during transport. Like the Medication Administration Record, it contains critical information including interventions administered, patient responses, and timestamped entries. Both forms ensure continuity of care by providing subsequent caregivers with a comprehensive view of prior treatments and responses.
Blood Glucose Tracking Chart: A chart used for tracking blood glucose levels at various times across the day, often by patients with diabetes. It shares similarities with the Medication Administration Record in terms of monitoring health parameters at different hours, facilitating the identification of patterns and adjustments in patient care. Both are vital tools in managing health conditions through close observation.
Dietary Intake Record: This form records all food and drink consumed by an individual over a specific period, similar to how medication intake is recorded. Both the Dietary Intake Record and the Medication Administration Record Sheet aim to monitor and analyze consumption patterns for health and treatment purposes, providing valuable insights for healthcare providers in devising care plans.
Vaccine Administration Record: This record tracks the vaccines an individual has received, including the date, type of vaccine, and dose. It mirrors the Medication Administration Record Sheet in its purpose to document and ensure that the necessary treatments are administered at the correct times and intervals, playing a crucial role in preventive healthcare.
Treatment Plan Documentation: Similar to the Medication Administration Record, this document outlines a patient's diagnosis, goals, and detailed treatments or interventions planned over a timeframe. Both documents are fundamental in planning and tracking healthcare interventions, ensuring that the care provided aligns with the individual’s health needs and progress towards goals.
When handling the Medication Administration Record Sheet (MAR), accuracy and diligence are paramount to ensure the well-being of the individual receiving medication. Below are lists of important dos and don'ts to consider when filling out this crucial document.
Things You Should Do
Things You Shouldn't Do
Adhering to these guidelines will contribute to the safe and effective management of medications, a responsibility that should never be taken lightly. Proper documentation is not only a regulatory requirement but also a cornerstone of quality healthcare provision.
Understanding the Medication Administration Record Sheet form is crucial for ensuring accurate documentation and administration of medications. However, there are some common misconceptions about this form that need to be clarified. Here are seven myths debunked:
By dispelling these misconceptions, caregivers and medical professionals can better understand the importance of accurately completing the Medication Administration Record Sheet. This document is a key tool in providing safe and effective care, ensuring that all medications are administered correctly and any changes in medication regimes are adequately recorded and communicated.
Filling out and using the Medication Administration Record Sheet is crucial in ensuring the proper management of medication for individuals in various healthcare settings. This document is designed to keep a detailed record of all medications administered to a person, tracking dosage, time, and the response to each medication. Here are key takeaways to remember about this form:
By keeping these key points in mind, caregivers and healthcare professionals can use the Medication Administration Record Sheet effectively to manage and monitor medication administration, contributing to the safety and well-being of individuals under their care.
Texas Hub Certification - Serves as a foundational document for understanding the distribution and movement of company equity among members.
Fl-300 Fillable Form - Ensure that the amounts deducted do not exceed federal consumer protection limits.