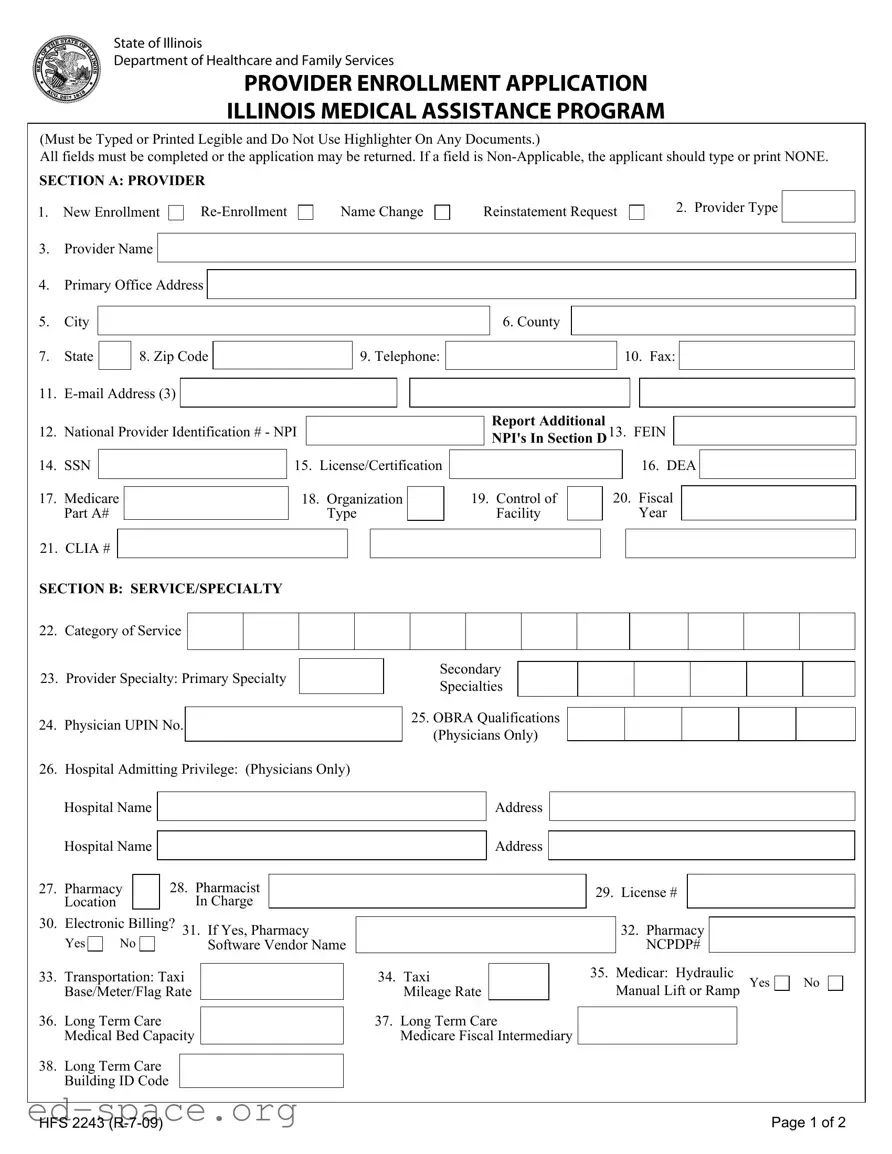
The Illinois HFS 2243 form is a critical document used for enrolling healthcare providers in the Illinois Medical Assistance Program. This form serves multiple purposes, including new enrollment, re-enrollment, name changes, and reinstatement requests. It requires providers to provide essential information, such as their name, address, and National Provider Identification (NPI) number, ensuring that all fields are completed accurately. The form is divided into several sections, each tailored to gather specific details about the provider's services, specialties, and any former participation in the program. For example, Section A focuses on basic provider information, while Section B delves into the categories of services and specialties offered. Additionally, Section E addresses payee information, which is vital for billing and reimbursement processes. Providers must also certify the accuracy of the information they provide, acknowledging the importance of compliance with federal and state regulations. Overall, the HFS 2243 form is a comprehensive tool that facilitates the enrollment process, ensuring that healthcare providers can participate effectively in the Illinois Medical Assistance Program.
State of Illinois
Department of Healthcare and Family Services
PROVIDER ENROLLMENT APPLICATION
ILLINOIS MEDICAL ASSISTANCE PROGRAM
(Must be Typed or Printed Legible and Do Not Use Highlighter On Any Documents.)
All fields must be completed or the application may be returned. If a field is
SECTION A: PROVIDER
1.New Enrollment
3.Provider Name
Name Change
Reinstatement Request
2. Provider Type
4.Primary Office Address
5.City
6. County
7.State
8. Zip Code
9. Telephone:
10. Fax:
11. |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
12. |
National Provider Identification # - NPI |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
14. |
SSN |
|
|
|
15. |
License/Certification |
|||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
||||
17. |
Medicare |
|
|
18. |
Organization |
|
|||
|
Part A# |
|
|
|
|
Type |
|
||
Report Additional
NPI's In Section D13. FEIN
|
|
|
16. DEA |
|
|
|
|
|
|
|
|
19. Control of |
|
20. Fiscal |
|
|
|
|
|
|
|||
Facility |
|
|
Year |
|
|
21. CLIA #
SECTION B: SERVICE/SPECIALTY
22.Category of Service
23.Provider Specialty: Primary Specialty
24.Physician UPIN No.
Secondary
Specialties
25.OBRA Qualifications (Physicians Only)
26. Hospital Admitting Privilege: (Physicians Only)
|
Hospital Name |
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hospital Name |
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
28. Pharmacist |
|
|
|
|
|
|
|
|
|
|
|
|||
27. |
Pharmacy |
|
|
|
|
|
|
|
|
29. |
License # |
|
|
|
|||
|
Location |
|
|
|
In Charge |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
30. |
Electronic Billing? 31. If Yes, Pharmacy |
|
|
|
|
|
32. Pharmacy |
|
|
||||||||
|
|
|
|
|
|
|
|||||||||||
|
Yes |
No |
|
Software Vendor Name |
|
|
|
|
|
NCPDP# |
|
|
|||||
33. |
Transportation: Taxi |
|
|
|
34. Taxi |
|
|
|
35. |
Medicar: Hydraulic |
|||||||
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
Manual Lift or Ramp Yes |
|||||||||||
|
Base/Meter/Flag Rate |
|
|
Mileage Rate |
|
|
|
|
|||||||||
36. |
Long Term Care |
|
|
|
|
37. Long Term Care |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
Medical Bed Capacity |
|
|
Medicare Fiscal Intermediary |
|
|
|
|
|
|
|||||||
38.Long Term Care Building ID Code
No
HFS 2243 |
Page 1 of 2 |
SECTION C: FORMER PARTICIPATION
39. Change of Ownership |
Yes |
40. Former Provider Number
No
Effective Date
Former Provider Name
SECTION D: ADDITIONAL NPI - National Provider Identification #
41. NPI
NPI
SECTION E: PAYEE INFORMATION
NPI
NPI
NPI
NPI
42. Name
44.DBA
45.Street Address
46.City
50.SSN/FEIN
52.Medicare Part B#
43. Telephone:
47. State |
|
|
|
48. Zip Code |
|
|
|
|
49. TIN Type Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
51. Billing Provider/Pay To NPI # |
|
|
|
|
|||
|
53. PIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
54. DMERC# |
|
|
|
|||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
Name
DBA
Street Address
Telephone:
City |
|
|
|
|
State |
|
|
Zip Code |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
SSN/FEIN |
|
|
|
|
|
|
Billing Provider/Pay To NPI # |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|||||
Medicare Part B# |
|
PIN |
|
|
|
|
|
DMERC# |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
SECTION F: CERTIFICATION/SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|||
TIN Type Code
I understand that knowingly falsifying or willfully withholding information may be cause for the denial or termination of participation in the Medical Assistance Program and such conduct may be prosecuted under applicable Federal and State laws..
Under penalties of perjury, I hereby certify that all of the information provided in this application process is true, correct and complete and that the enrolling provider is in compliance with all applicable federal and state laws and regulations. I further certify that neither I, nor any of the following provider's employees, partners, officers, or shareholders owning at least five percent (5%) of said provider are currently barred, suspended, terminated, voluntarily withdrawn as part of a settlement agreement, or otherwise excluded from participation in the Medicaid or Medicare programs, nor are any of the above currently under sanction for, or serving a sentence for conviction of any Medicaid or Medicare program violations. I further certify that none of the above are currently sanctioned by any federal agency for any reason. I authorize the Department of Healthcare and Family Services, to verify the information provided on this application with other state and federal agencies. I further certify that I will review and comply with the Department's policies, rules and regulations including but not limited to those found at the following websites:
Illinois HFS website address: http://www.hfs.illinois.gov/
Illinois HFS Handbook updates are available: http://www.hfs.illinois.gov/handbooks
Illinois HFS Laws and Rule Regulations: http://www.hfs.illinois.gov/lawsrules/index.html
Signature:
Printed name of person signing above
Check this box if you want a provider handbook mailed
Date
HFS 2243 |
Page 2 of 2 |
| Fact Name | Details |
|---|---|
| Form Title | Provider Enrollment Application for the Illinois Medical Assistance Program. |
| Governing Law | This form is governed by the Illinois Public Aid Code (305 ILCS 5). |
| Completion Requirement | All fields must be completed. Inapplicable fields should be marked as "NONE." |
| Submission Format | The application must be typed or printed legibly. Avoid using highlighters. |
| Provider Types | Includes categories like new enrollment, re-enrollment, name change, and reinstatement requests. |
| Primary Information | Requires essential details such as provider name, address, and contact information. |
| National Provider Identification | Providers must include their National Provider Identification (NPI) number on the form. |
| Certification Requirement | The signer must certify the truthfulness of the information and compliance with relevant laws. |
| Electronic Billing Option | Providers must indicate if they utilize electronic billing and provide vendor information if applicable. |
Completing the Illinois HFS 2243 form is a crucial step in the provider enrollment process for the Illinois Medical Assistance Program. After filling out the form, it will need to be submitted to the appropriate department for processing. Ensure that all information is accurate and complete to avoid delays.
What is the purpose of the Illinois HFS 2243 form?
The Illinois HFS 2243 form serves as a provider enrollment application for the Illinois Medical Assistance Program. This form is essential for healthcare providers who wish to participate in the program, allowing them to provide services to Medicaid recipients. Completing this form accurately is crucial for ensuring that the application is processed without delays.
Who needs to fill out the HFS 2243 form?
Healthcare providers who are seeking to enroll in the Illinois Medical Assistance Program must complete the HFS 2243 form. This includes new providers, those re-enrolling, changing their name, or requesting reinstatement. It is also necessary for providers who have undergone a change of ownership.
What information is required on the HFS 2243 form?
The form requires a variety of information, including the provider's name, type, primary office address, contact details, and National Provider Identification (NPI) number. Additionally, it asks for information regarding the provider's specialties, licenses, and any former participation in the program. Every field must be completed, or the application may be returned.
What should I do if a field is not applicable to me?
If any field on the form does not apply to you, it is important to type or print "NONE" in that section. This practice helps clarify that the field was intentionally left blank rather than overlooked, ensuring that your application is complete and can be processed efficiently.
How can I submit the HFS 2243 form?
The completed HFS 2243 form can typically be submitted by mail or electronically, depending on the specific instructions provided by the Illinois Department of Healthcare and Family Services. Ensure that you follow the submission guidelines carefully to avoid any issues with your application.
What happens if I make a mistake on the form?
Should you discover a mistake after submitting the form, it is advisable to contact the Illinois Department of Healthcare and Family Services as soon as possible. They can guide you on the appropriate steps to correct the error, which may involve submitting an amended application or providing additional documentation.
Is there a deadline for submitting the HFS 2243 form?
While specific deadlines may vary depending on individual circumstances or changes in regulations, it is generally best to submit the HFS 2243 form as soon as possible. Delays in submission could affect your ability to participate in the Medical Assistance Program and provide services to Medicaid recipients.
Where can I find additional resources or assistance regarding the HFS 2243 form?
For more information, you can visit the Illinois Department of Healthcare and Family Services website. They provide resources, including handbooks and guidelines, to assist providers in completing the HFS 2243 form and understanding the enrollment process. Additionally, reaching out to their customer service can provide personalized assistance.
Incomplete Fields: One common mistake is leaving fields blank. Every section of the Illinois HFS 2243 form must be completed. If a field does not apply, applicants should type or print "NONE" to indicate that it is not applicable.
Using Highlighters: Many applicants mistakenly use highlighters on the form. The instructions clearly state that highlighters should not be used on any documents submitted with the application. This can lead to issues with readability and processing.
Incorrect Provider Information: Failing to provide accurate provider information is another frequent error. This includes details such as the provider's name, National Provider Identification number, and contact information. Any discrepancies can delay the enrollment process.
Not Signing the Form: Some applicants overlook the importance of signing the form. The certification/signature section is crucial, as it verifies that the information provided is true and complete. Without a signature, the application may be rejected.
When submitting the Illinois HFS 2243 form for provider enrollment in the Illinois Medical Assistance Program, several other documents may also be required. These documents help ensure that all necessary information is provided and assist in the enrollment process. Below is a list of common forms and documents often used alongside the HFS 2243 form.
Each of these documents plays a crucial role in the enrollment process, helping to ensure that all necessary information is accurately provided. It is important to complete and submit each form carefully to avoid delays in the application process.
The Illinois HFS 2243 form is an important document for healthcare providers looking to enroll in the Illinois Medical Assistance Program. Several other documents serve similar purposes and share characteristics with the HFS 2243 form. Here are four such documents:
When completing the Illinois HFS 2243 form, it’s important to follow certain guidelines to ensure your application is processed smoothly. Here’s a list of things you should and shouldn’t do:
Following these guidelines can help avoid delays and ensure your application is processed correctly. Always double-check your information before submitting the form to the Illinois Department of Healthcare and Family Services.
Misconceptions about the Illinois HFS 2243 form can lead to confusion and mistakes during the application process. Here are eight common misunderstandings:
Filling out the Illinois HFS 2243 form is an essential step for healthcare providers seeking enrollment in the Illinois Medical Assistance Program. Here are key takeaways to consider:
By following these guidelines, healthcare providers can streamline the enrollment process and ensure compliance with the requirements set forth by the Illinois Department of Healthcare and Family Services.