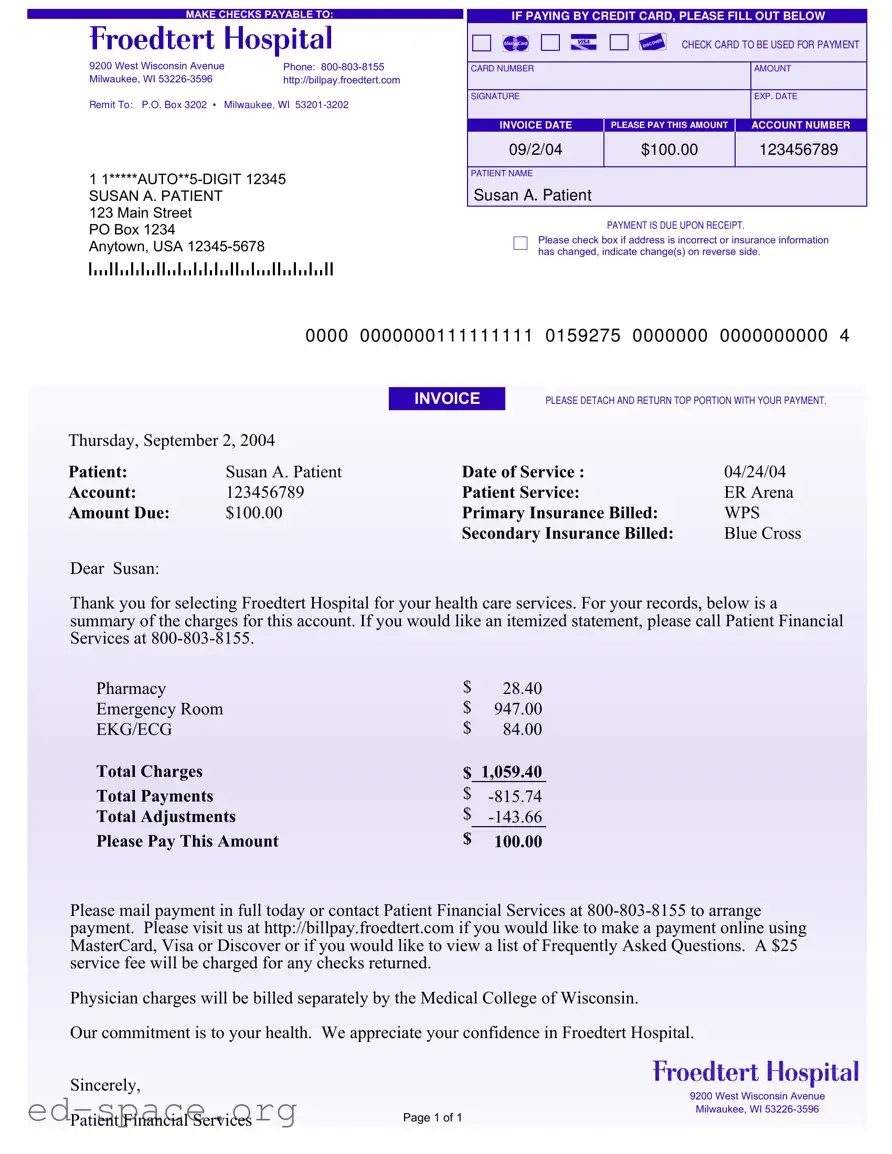
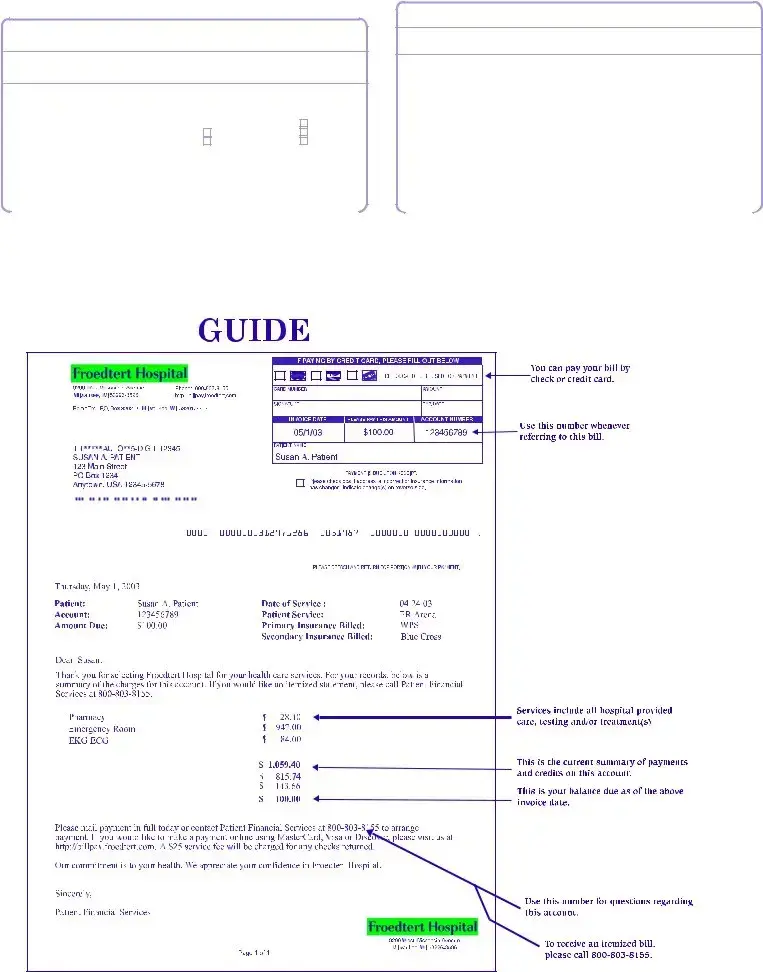
The Hospital Bill form is a crucial document that patients receive after receiving medical services, providing a clear summary of charges and payment obligations. This form typically includes essential details such as the patient's name, account number, and date of service, ensuring that individuals can easily identify their specific bill. It outlines the total charges incurred, including itemized costs for various services, such as emergency room visits, pharmacy fees, and diagnostic tests. Additionally, the form highlights any payments made and adjustments applied, ultimately presenting the amount due. Patients are encouraged to remit payment promptly, with clear instructions for both mailing a check and paying online using credit cards. Moreover, the form offers a section for updating personal and insurance information, which is vital for maintaining accurate records. Overall, the Hospital Bill form serves as a comprehensive tool for managing healthcare expenses while fostering transparency and communication between patients and the healthcare provider.
MAKE CHECKS PAYABLE TO:
9200 West Wisconsin Avenue |
Phone: |
Milwaukee, WI |
http://billpay.froedtert.com |
Remit To: P.O. Box 3202 • Milwaukee, WI
1
SUSAN A. PATIENT
123 Main Street
PO Box 1234
Anytown, USA
IF PAYING BY CREDIT CARD, PLEASE FILL OUT BELOW
CHECK CARD TO BE USED FOR PAYM ENT
CARD NUMBER |
AMOUNT |
|
|
SIGNATURE |
EXP. DATE |
|
|
INVOICE DATE |
PLEASE PAY THIS AMOUNT |
ACCOUNT NUMBER |
09/2/04 |
$100.00 |
123456789 |
|
|
|
PATIENT NAME
Susan A. Patient
PAYMENT IS DUE UPON RECEIPT.
Please check box if address is incorrect or insurance information has changed, indicate change(s) on reverse side.
|
0000 |
0000000111111111 |
0159275 |
0000000 |
0000000000 |
4 |
|
|
INVOICE |
PLEASE DETACH AND RETURN TOP PORTION WITH YOUR PAYMENT. |
|
||
Thursday, September 2, 2004 |
|
|
|
|
|
|
Patient: |
Susan A. Patient |
Date of Service : |
|
04/24/04 |
|
|
Account: |
123456789 |
Patient Service: |
|
ER Arena |
|
|
Amount Due: |
$100.00 |
Primary Insurance Billed: |
WPS |
|
||
|
|
Secondary Insurance Billed: |
Blue Cross |
|
||
Dear Susan:
Thank you for selecting Froedtert Hospital for your health care services. For your records, below is a summary of the charges for this account. If you would like an itemized statement, please call Patient Financial Services at
Pharmacy |
$ |
28.40 |
Emergency Room |
$ |
947.00 |
EKG/ECG |
$ |
84.00 |
Total Charges |
$ |
1,059.40 |
Total Payments |
$ |
|
Total Adjustments |
$ |
|
Please Pay This Amount |
$ |
100.00 |
Please mail payment in full today or contact Patient Financial Services at
Physician charges will be billed separately by the Medical College of Wisconsin.
Our commitment is to your health. We appreciate your confidence in Froedtert Hospital.
Sincerely,
9200 West Wisconsin Avenue
|
Milwaukee, WI |
Patient Financial Services |
Page 1 of 1 |
|
PLEASE UPDATE ANY INFORM ATION THAT HAS CHANGED SINCE YOUR LAST STATEM ENT
ABOUT YOU:
YOUR NAME (Last, First, Middle Initial)
ADDRESS
CITY |
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
|
|
ZIP |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
|
|
|
|
|
|
|
|
|
MARITAL STATUS |
|
|
|
|
Separated |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single |
|
|
|
|
Divorced |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Married |
|
|
|
|
Widowed |
|
||||||
EMPLOYER'S NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER'S ADDRESS |
|
|
|
|
|
|
|
CITY |
STATE |
|
|
|
|
ZIP |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ABOUT YOUR INSURANCE:
YOUR PRIMARY INSURANCE COMPANY'S NAME
PRIMARY INSURANCE COMPANY'S ADDRESS
CITY |
STATE |
ZIP |
||
|
|
|
|
|
POLICYHOLDER'S ID NUMBER |
GROUP PLAN NUMBER |
|
|
|
|
|
|
|
|
YOUR SECONDARY INSURANCE COMPANY'S NAME |
|
|
|
|
|
|
|
|
|
SECONDARY INSURANCE COMPANY'S ADDRESS |
|
|
|
|
|
|
|
|
|
CITY |
STATE |
ZIP |
||
|
|
|
|
|
POLICYHOLDER'S ID NUMBER |
GROUP PLAN NUMBER |
|
|
|
|
|
|
|
|
| Fact Name | Details |
|---|---|
| Payable To | Checks should be made payable to Froedtert Hospital. |
| Contact Information | The hospital's phone number is 800-803-8155. |
| Mailing Address | Payments should be sent to P.O. Box 3202, Milwaukee, WI 53201-3202. |
| Payment Methods | Payments can be made by credit card, check, or online. |
| Invoice Date | The invoice date is September 2, 2004. |
| Amount Due | The total amount due is $100.00. |
| Insurance Information | Primary insurance billed is WPS; secondary is Blue Cross. |
| Service Fee | A $25 service fee applies for any returned checks. |
| Itemized Statement | For an itemized statement, contact Patient Financial Services. |
| Legal Compliance | This form adheres to Wisconsin's healthcare billing regulations. |
Filling out the Hospital Bill form is a straightforward process. By following these steps, you can ensure that your payment is processed efficiently. Make sure to have all necessary information on hand before you begin.
Once you have submitted the form, you can expect to receive confirmation of your payment. If you have any questions or need assistance, do not hesitate to contact Patient Financial Services at the provided phone number.
What should I do if I receive a hospital bill form?
When you receive a hospital bill form, it is important to review it carefully. Check that all the information is accurate, including your name, address, and the services rendered. If you notice any discrepancies, contact Patient Financial Services at 800-803-8155 for assistance. They can help clarify any questions you may have about your bill.
How can I make a payment on my hospital bill?
You can make a payment in several ways. If you prefer to pay by mail, send your payment to the address listed on the form: P.O. Box 3202, Milwaukee, WI 53201-3202. Make checks payable to the hospital. Alternatively, you can pay online at http://billpay.froedtert.com using a credit card such as MasterCard, Visa, or Discover.
What if I want an itemized statement of my charges?
If you would like a detailed breakdown of your charges, you can request an itemized statement. Simply call Patient Financial Services at 800-803-8155, and they will provide you with the necessary information.
What happens if I do not pay my bill on time?
Payment is due upon receipt of the bill. If you do not pay on time, you may incur late fees or additional charges. It's advisable to pay promptly to avoid complications. If you are experiencing financial difficulties, reach out to Patient Financial Services to discuss potential payment arrangements.
Can I update my personal or insurance information on the bill form?
Yes, the bill form includes a section for you to update any changes in your personal or insurance information. Fill out the relevant fields with the correct information, and return the top portion of the form with your payment.
What should I do if I have insurance?
If you have insurance, the hospital will bill your primary and secondary insurance companies directly. Ensure that the insurance information on the bill form is correct. If you have any questions about your coverage or what is billed, contact your insurance provider or Patient Financial Services for assistance.
Is there a fee for returned checks?
Yes, there is a $25 service fee for any checks that are returned. To avoid this fee, ensure that you have sufficient funds in your account before issuing a check for payment.
Who can I contact if I have questions about my bill?
If you have questions regarding your bill, you can contact Patient Financial Services at 800-803-8155. They can assist you with inquiries about charges, payments, and any other billing concerns you may have.
What if I believe there is an error on my bill?
If you suspect there is an error on your bill, it is crucial to address it promptly. Contact Patient Financial Services as soon as possible to discuss your concerns. They will review your account and help resolve any discrepancies.
Are physician charges included in the hospital bill?
No, physician charges are billed separately by the Medical College of Wisconsin. You will receive a separate bill for any physician services. If you have questions about these charges, you should contact the Medical College of Wisconsin directly.
Not including the correct payment amount. Always double-check the total due to avoid underpayment or overpayment.
Forgetting to fill out the credit card information if paying by card. Ensure you complete all required fields, including the card number and expiration date.
Leaving the signature field blank. A signature is necessary to authorize the payment.
Neglecting to update personal information. If your address or insurance details have changed, make sure to indicate those changes.
Not checking the box for incorrect address. If your address is wrong, this box should be marked to prevent issues with future correspondence.
Failing to include insurance information. If you have insurance, provide all necessary details to ensure proper billing.
Overlooking the invoice date. Always confirm that the date is correct to avoid confusion with payment deadlines.
Not detaching the top portion of the bill. This part needs to be sent back with your payment for proper processing.
Ignoring the service fee notice. Be aware that a fee may apply if your check is returned.
Submitting the form without making a copy for your records. Keeping a copy is essential for tracking your payments.
When dealing with hospital billing and payment processes, several forms and documents complement the Hospital Bill form. Each of these documents plays a crucial role in ensuring accurate billing, payment processing, and communication between the hospital and the patient. Below is a list of commonly used forms and documents.
Understanding these documents can streamline the billing process and facilitate effective communication between patients and healthcare providers. Keeping these forms organized and accessible is beneficial for managing healthcare expenses efficiently.
When filling out the Hospital Bill form, it’s important to be careful and thorough. Here are some things you should and shouldn’t do:
Following these steps will help ensure that your bill is processed smoothly and without delays.
Misconceptions about the Hospital Bill form can lead to confusion regarding payment responsibilities and processes. Here are four common misconceptions:
When filling out and using the Hospital Bill form, consider the following key takeaways: