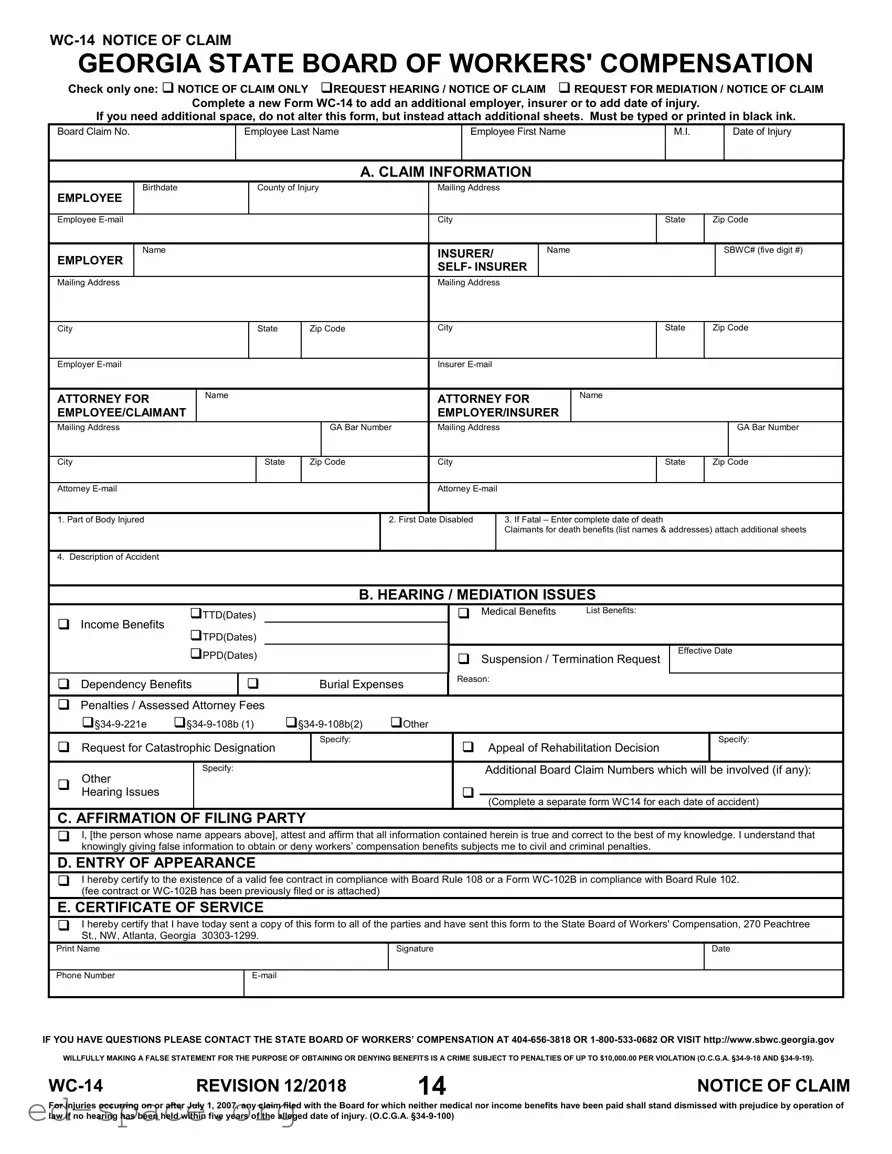
The Georgia WC-14 form is a crucial document in the workers' compensation process, serving multiple purposes for employees, employers, and insurers. It allows individuals to formally notify the Georgia State Board of Workers' Compensation about a claim. Users can select from various options, including submitting a notice of claim only, requesting a hearing, or seeking mediation. The form requires detailed information about the employee, including their name, birthdate, and mailing address, as well as specifics about the injury, such as the date it occurred and the part of the body affected. It also includes sections for the employer's and insurer's details, ensuring that all parties are properly identified. Additionally, the WC-14 form addresses various issues related to the claim, such as temporary total disability, medical benefits, and dependency benefits. A key feature is the affirmation section, where the filer attests to the accuracy of the information provided, highlighting the seriousness of submitting false statements. Finally, the form mandates a certificate of service, confirming that all relevant parties have been notified. This comprehensive approach ensures that the claims process is transparent and accountable.
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
Check only one: NOTICE OF CLAIM ONLY REQUEST HEARING / NOTICE OF CLAIM REQUEST FOR MEDIATION / NOTICE OF CLAIM
Complete a new Form
If you need additional space, do not alter this form, but instead attach additional sheets. Must be typed or printed in black ink.
Board Claim No.
Employee Last Name
Employee First Name
M.I.
Date of Injury
A. CLAIM INFORMATION
EMPLOYEE
Birthdate
County of Injury
Mailing Address
Employee
City
State
Zip Code
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
INSURER/ |
|
Name |
|
|
|
|
|
SBWC# (five digit #) |
||||
EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
SELF- INSURER |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
State |
Zip Code |
City |
|
|
|
|
|
|
State |
Zip Code |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Employer |
|
|
|
|
|
|
|
|
|
Insurer |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ATTORNEY FOR |
|
Name |
|
|
|
ATTORNEY FOR |
Name |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
EMPLOYEE/CLAIMANT |
|
|
|
|
|
|
|
|
|
EMPLOYER/INSURER |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Mailing Address |
|
|
|
|
|
|
|
GA Bar Number |
Mailing Address |
|
|
|
|
|
|
|
|
GA Bar Number |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City |
|
|
|
|
|
State |
Zip Code |
City |
|
|
|
|
|
|
State |
Zip Code |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Attorney |
|
|
|
|
|
|
|
|
|
Attorney |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
1. Part of Body Injured |
|
|
|
|
|
|
|
|
2. First Date Disabled |
|
|
3. If Fatal – Enter complete date of death |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Claimants for death benefits (list names & addresses) attach additional sheets |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. Description of Accident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
B. HEARING / MEDIATION ISSUES |
|
|
|
|
|
|||||||||
|
|
TTD(Dates) |
|
|
|
|
|
|
Medical Benefits |
List Benefits: |
|
|
|
|
|
||||||||
Income Benefits |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
TPD(Dates) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
PPD(Dates) |
|
|
|
|
Suspension / Termination Request |
|
Effective Date |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
Reason: |
|
|
|
|
|
|
|
|
|
||
Dependency Benefits |
|
|
Burial Expenses |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Penalties / Assessed Attorney Fees
|
Other |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Request for Catastrophic Designation |
|
Specify: |
|
|
Appeal of Rehabilitation Decision |
Specify: |
||
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Other |
|
Specify: |
|
|
|
|
Additional Board Claim Numbers which will be involved (if any): |
|
|
|
|
|
|
|
|
|
|
|
|
Hearing Issues |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Complete a separate form WC14 for each date of accident) |
|||
|
|
|
|
|
|
|
|||
C. AFFIRMATION OF FILING PARTY
I, [the person whose name appears above], attest and affirm that all information contained herein is true and correct to the best of my knowledge. I understand that knowingly giving false information to obtain or deny workers’ compensation benefits subjects me to civil and criminal penalties.
D. ENTRY OF APPEARANCE
I hereby certify to the existence of a valid fee contract in compliance with Board Rule 108 or a Form
E. CERTIFICATE OF SERVICE
I hereby certify that I have today sent a copy of this form to all of the parties and have sent this form to the State Board of Workers' Compensation, 270 Peachtree St., NW, Atlanta, Georgia
Print Name
Signature
Date
Phone Number
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION 12/2018 |
14 |
NOTICE OF CLAIM |
For injuries occurring on or after July 1, 2007, any claim filed with the Board for which neither medical nor income benefits have been paid shall stand dismissed with prejudice by operation of law if no hearing has been held within five years of the alleged date of injury. (O.C.G.A.
| Fact Name | Details |
|---|---|
| Form Purpose | The WC-14 form is used to notify the Georgia State Board of Workers' Compensation of a claim. |
| Submission Options | Claimants can submit a notice of claim only, request a hearing, or request mediation. |
| Completing the Form | The form must be typed or printed in black ink. Additional sheets may be attached if more space is needed. |
| Claimant Information | Essential information includes the employee's name, date of injury, and mailing address. |
| Injury Details | Claimants must specify the part of the body injured and the first date of disability. |
| Filing Affirmation | Filing parties must affirm the truthfulness of the information provided, acknowledging penalties for false statements. |
| Attorney Certification | Attorneys must certify the existence of a valid fee contract or attach a Form WC-102B. |
| Certificate of Service | Claimants must certify that a copy of the form has been sent to all parties and the State Board. |
| Governing Laws | The form is governed by O.C.G.A. §34-9-18, §34-9-19, and §34-9-100. |
Completing the Georgia WC-14 form is a critical step in the workers' compensation process. After filling out this form, you will need to submit it to the State Board of Workers' Compensation and send copies to all relevant parties. Make sure to double-check your entries for accuracy, as errors can lead to delays in processing your claim.
What is the purpose of the Georgia WC-14 form?
The Georgia WC-14 form serves as a notice of claim for workers' compensation. It allows employees or their representatives to formally notify the State Board of Workers' Compensation about a claim related to a workplace injury. The form can also be used to request a hearing or mediation regarding the claim. Proper completion of this form is essential for ensuring that all relevant parties are informed and that the claim is processed efficiently.
Who should fill out the WC-14 form?
The WC-14 form should be filled out by the employee or their attorney if they are seeking to claim benefits for a work-related injury. It can also be completed by the employer or insurer if they are responding to a claim. Each party must provide accurate information regarding the injury, including details about the employee, the employer, and the nature of the claim.
What information is required on the WC-14 form?
Essential information on the WC-14 form includes the employee's name, birthdate, mailing address, and details about the injury, such as the date of injury and part of the body injured. Additionally, the form requires information about the employer and insurer, including their names and contact details. Any claims for specific benefits, such as medical or income benefits, must also be indicated on the form.
How do I submit the WC-14 form?
Once the WC-14 form is completed, it must be submitted to the State Board of Workers' Compensation. This can be done by mailing the form to the address provided on the form or by delivering it in person. It is crucial to ensure that a copy of the form is sent to all involved parties, as certification of this action is required on the form itself.
What happens if I do not file the WC-14 form within the required time frame?
If the WC-14 form is not filed within the specified time frame, the claim may be dismissed. For injuries occurring on or after July 1, 2007, if no hearing has been held within five years of the alleged date of injury, the claim will be dismissed with prejudice by operation of law. This means that the claim cannot be refiled, underscoring the importance of timely submission.
What are the consequences of providing false information on the WC-14 form?
Providing false information on the WC-14 form can lead to serious legal repercussions. Willfully making a false statement to obtain or deny workers' compensation benefits is considered a crime and can result in penalties of up to $10,000 per violation. It is vital to ensure that all information provided is accurate and truthful to avoid these severe consequences.
Failing to check the correct box for the type of claim being filed. Choose only one option: Notice of Claim Only, Request Hearing / Notice of Claim, or Request for Mediation / Notice of Claim.
Not providing complete information about the employee, including the last name, first name, and middle initial. Missing details can delay processing.
Leaving out the date of injury. This is crucial for establishing the timeline of the claim.
Using incorrect ink color. The form must be typed or printed in black ink only.
Not including the complete mailing addresses for the employer, insurer, and attorney. Incomplete addresses can hinder communication.
Failing to list all necessary parties involved in the claim. This includes the names and addresses of claimants for death benefits, if applicable.
Neglecting to specify the type of benefits being claimed. Clearly indicate whether you are requesting TTD, TPD, PPD, or other benefits.
Not providing an accurate description of the accident. This section is vital for understanding the circumstances surrounding the claim.
Overlooking the affirmation section. The form must be signed and dated by the filing party to validate the claim.
Failing to send copies of the form to all relevant parties and the State Board of Workers' Compensation. Ensure compliance with the Certificate of Service.
The Georgia WC-14 form is a crucial document for initiating a workers' compensation claim. It serves as a notice of claim and can also request a hearing or mediation. When completing the WC-14, several other forms may be necessary to support your claim or address specific issues. Below is a list of commonly used forms and documents that complement the WC-14.
Each of these forms plays a vital role in the workers' compensation process in Georgia. Properly completing and submitting the necessary documentation can significantly impact the outcome of a claim. Understanding these forms will help ensure that all parties are informed and that the process runs smoothly.
Filling out the Georgia WC-14 form correctly is essential for ensuring your claim is processed smoothly. Here are five important things to do and avoid when completing this form.
This is not true. The WC-14 form can also be used to add additional employers or insurers, or to update the date of injury. It serves multiple purposes beyond just initiating a new claim.
Altering the form is not allowed. If you need more space, you should attach additional sheets instead. This keeps the process organized and ensures all information is clearly presented.
Submitting the form is just one step. After filing, you may need to participate in hearings or mediation sessions. The process can involve multiple stages, depending on the specifics of your case.
While it primarily addresses injuries, the form can also be used for claims related to fatalities. In such cases, additional information about the deceased and dependents must be provided.
This is incorrect. You must certify that you have sent copies of the form to all involved parties, including the State Board of Workers' Compensation. This ensures transparency and keeps everyone informed.
When filling out the Georgia WC-14 form, it’s essential to pay attention to the details. Here are some key takeaways to keep in mind:
Following these guidelines can help ensure that your claim is processed efficiently and accurately.