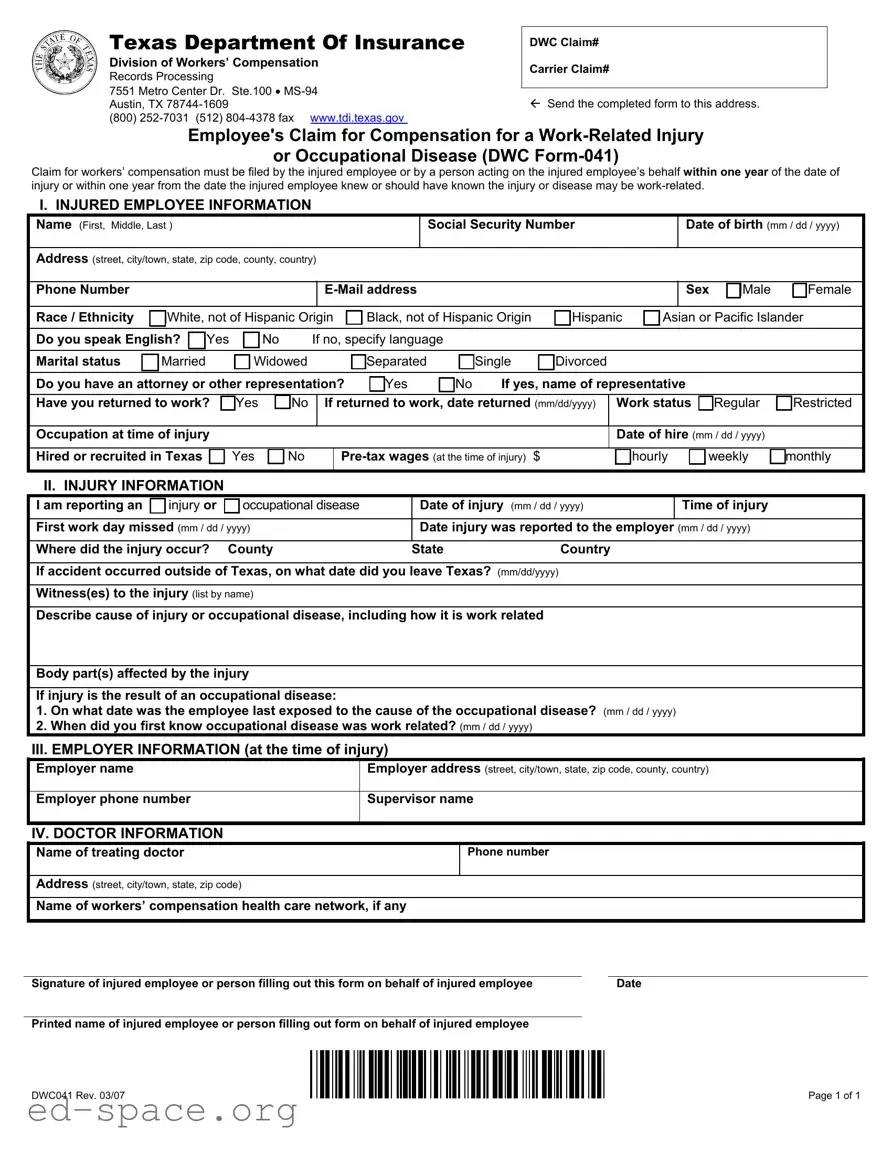
The DWC Form-041, officially titled the Employee's Claim for Compensation for a Work-Related Injury or Occupational Disease, is a crucial document for employees seeking workers' compensation benefits in Texas. This form must be completed and submitted by the injured employee or an authorized representative within one year of the injury date or the date the employee became aware of a work-related condition. Key sections of the form include personal information about the injured employee, details regarding the injury or occupational disease, and information about the employer at the time of the incident. Additionally, it requires the name and contact information of the treating doctor. Proper completion of the form is essential, as it initiates the claims process with the Texas Department of Insurance, Division of Workers’ Compensation. Upon receipt, the Division will assign a claim number and provide necessary information regarding the claims process to both the employee and their employer's insurance carrier. Adhering to the guidelines and ensuring all sections are filled out accurately can significantly impact the outcome of the claim.
Texas Department Of Insurance
Division of Workers’ Compensation
Records Processing
7551 Metro Center Dr. Ste.100 •
(800)
DWC Claim#
Carrier Claim#
Send the completed form to this address.
Employee's Claim for Compensation for a
or Occupational Disease (DWC
Claim for workers’ compensation must be filed by the injured employee or by a person acting on the injured employee’s behalf within one year of the date of injury or within one year from the date the injured employee knew or should have known the injury or disease may be
I. INJURED EMPLOYEE INFORMATION
Name (First, Middle, Last )
Social Security Number
Date of birth (mm / dd / yyyy)
Address (street, city/town, state, zip code, county, country)
Phone Number
Sex Male Female
Race / Ethnicity |
White, not of Hispanic Origin |
Black, not of Hispanic Origin |
Hispanic |
Asian or Pacific Islander |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Yes |
No |
|
|
If no, specify language |
|
|
|
|
|
|
|
|
||||||||
Do you speak English? |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Married |
|
Widowed |
|
|
|
|
Separated |
Single |
Divorced |
|
|
|
|
|
|||||||
Marital status |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Do you have an attorney or other representation? |
Yes |
No |
If yes, name of representative |
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Have you returned to work? |
Yes |
|
|
No |
|
If returned to work, date returned (mm/dd/yyyy) |
|
Work status |
Regular |
Restricted |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupation at time of injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of hire (mm / dd / yyyy) |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Hired or recruited in Texas |
|
Yes |
No |
|
|
|
|
|
hourly |
weekly |
monthly |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
II. INJURY INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
I am reporting an |
injury or |
occupational disease |
|
Date of injury (mm / dd / yyyy) |
|
|
Time of injury |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
First work day missed (mm / dd / yyyy) |
|
|
|
|
|
|
|
Date injury was reported to the employer (mm / dd / yyyy) |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Where did the injury occur? County |
|
|
|
|
|
|
|
State |
|
Country |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
If accident occurred outside of Texas, on what date did you leave Texas? (mm/dd/yyyy) |
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Witness(es) to the injury (list by name) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Describe cause of injury or occupational disease, including how it is work related |
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Body part(s) affected by the injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
If injury is the result of an occupational disease: |
|
|
|
|
|
|
|
|
|
|
||||||||||||
1. On what date was the employee last exposed to the cause of the occupational disease? (mm / dd / yyyy) |
|
|
||||||||||||||||||||
2. When did you first know occupational disease was work related? (mm / dd / yyyy) |
|
|
|
|
|
|
|
|||||||||||||||
III. EMPLOYER INFORMATION (at the time of injury) |
|
|
|
|
|
|
|
|
|
|||||||||||||
Employer name |
|
|
|
|
|
|
|
|
|
|
|
Employer address (street, city/town, state, zip code, county, country) |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Employer phone number |
|
|
|
|
|
|
|
|
|
Supervisor name |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IV. DOCTOR INFORMATION
|
Name of treating doctor |
Phone number |
|
|
|
|
|
|
|
|
|
|
|
|
Address (street, city/town, state, zip code) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of workers’ compensation health care network, if any |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of injured employee or person filling out this form on behalf of injured employee |
|
Date |
|
||
|
|
|
|
|
|
|
|
Printed name of injured employee or person filling out form on behalf of injured employee |
|
|
|
||
|
|
|
|
|
|
|
|
DWC041 Rev. 03/07 |
|
|
|
Page 1 of 1 |
|
Information about Employee's Claim for Compensation for a
Injury or Occupational Disease (DWC
A claim for Workers' Compensation benefits must be filed with the Division of Workers’ Compensation (Division) by the injured employee (you), or by a person acting on the injured employee's (your) behalf within one year of the injury or within one year from the date you knew or should have known the injury or disease may be work related;
UNLESS good cause exists for the failure to timely file a claim, or the employer or the employer's insurance carrier does not contest the claim.
Upon receipt of your completed DWC
SPECIAL INSTRUCTIONS AND INFORMATION FOR COMPLETING THE DWC
General Instructions
•Complete all boxes in the DWC
•If you have questions about completing this form, please call your local Division Field Office at
Injured Employee Information
•Work Status information
OIf you have returned to your regular job and you are performing the same duties as you were before your injury, check the “Regular” box.
OIf you have been released to work with restrictions by a doctor, check “Restricted.”
Injury Information
•An injury is damage to your body that was caused by a single incident, accident, or event.
•An occupational disease is an illness or injury related to or caused by the work you do, and may include injuries to your body that are the result of repetitive activities you performed on the job over a period of time.
Employer Information
•Provide information about your employer at the time you were injured.
Doctor Information
•If you already have a workers’ compensation treating doctor, provide the name and address of the doctor.
•If you are covered under a workers’ compensation healthcare network, provide the name of the network.
Contacting Texas Department of Insurance, Division of Workers’ Compensation
If you have questions about filling out this form or workers’ compensation in Texas, please call your local Division Field Office at
NOTE: With few exceptions, you are entitled, on request, to be informed about the information that the Division collects or maintains about you and your workers’ compensation claim. Under §552.021 and 552.023 of the Texas Government Code, you are entitled to receive and review the information. Under §559.004 of the Texas Government Code you are entitled to have the Division correct information the Division creates about you or your workers’ compensation claim that is incorrect. For more information, call the Division’s Open Records section at
DWC041 Rev. 03/07 |
Instructions |
| Fact Name | Description |
|---|---|
| Form Purpose | The DWC Form-041 is used by employees to claim compensation for work-related injuries or occupational diseases. |
| Filing Deadline | Claims must be filed within one year of the injury or when the employee knew or should have known the injury was work-related. |
| Governing Law | This form is governed by the Texas Workers' Compensation Act, specifically under Title 5 of the Texas Labor Code. |
| Who Can File | The injured employee or a representative acting on their behalf can file the claim. |
| Submission Address | The completed form should be sent to the Texas Department of Insurance, Division of Workers’ Compensation at 7551 Metro Center Dr. Ste. 100, Austin, TX 78744-1609. |
| Contact Information | For questions, individuals can call 1-800-252-7031 or fax to (512) 804-4378. |
| Information Required | Essential information includes the employee's personal details, injury specifics, and employer information. |
| Work Status | Employees must indicate their work status, whether regular or restricted, at the time of filing. |
| Occupational Disease | If claiming an occupational disease, additional details about exposure and awareness of the condition are required. |
| Record Access Rights | Employees have the right to access and request corrections to their information under the Texas Government Code. |
Filling out the DWC 041 form is an essential step in initiating your claim for workers' compensation benefits. This form must be completed accurately to ensure that your claim is processed smoothly. Once you have filled out the form, it should be sent to the Texas Department of Insurance, Division of Workers’ Compensation at the specified address.
What is the DWC 041 form?
The DWC 041 form, also known as the Employee's Claim for Compensation for a Work-Related Injury or Occupational Disease, is a document used in Texas to file a claim for workers' compensation benefits. It must be completed by the injured employee or someone acting on their behalf within one year of the injury or the date they became aware that the injury might be work-related.
Who needs to fill out the DWC 041 form?
This form needs to be filled out by the injured employee or a representative acting on their behalf. It is essential for those who have sustained a work-related injury or occupational disease and wish to claim workers' compensation benefits.
Where should the completed DWC 041 form be sent?
The completed DWC 041 form should be sent to the Texas Department of Insurance, Division of Workers’ Compensation, at 7551 Metro Center Dr. Ste. 100, MS-94, Austin, TX 78744-1609. You may also contact them at (800) 252-7031 for further assistance.
What information is required on the DWC 041 form?
The form requires various details, including the injured employee's personal information, the specifics of the injury or occupational disease, employer information at the time of the injury, and the name of the treating doctor. It is important to provide accurate and complete information to avoid delays in processing the claim.
What happens after I submit the DWC 041 form?
Once the Division receives the completed DWC 041 form, they will create a claim and assign a DWC claim number. You will receive information regarding workers' compensation in Texas, and your employer and their insurance carrier will also be notified of your claim.
What is the deadline for filing the DWC 041 form?
The form must be filed within one year of the injury date or within one year from when the injured employee knew or should have known that the injury or disease was work-related. Exceptions may apply if there is good cause for the delay or if the employer or their insurance carrier does not contest the claim.
What if I have questions about filling out the DWC 041 form?
If you have questions or need assistance with completing the DWC 041 form, you can call your local Division Field Office at 1-800-252-7031. They can provide guidance and clarify any uncertainties you may have.
Do I need an attorney to file the DWC 041 form?
While it is not mandatory to have an attorney to file the DWC 041 form, having legal representation can be beneficial, especially if your claim is complex or if you encounter disputes. If you have an attorney, you should indicate their name on the form.
What if my injury is the result of an occupational disease?
If your injury is classified as an occupational disease, you will need to provide additional details on the form. This includes the date of last exposure to the cause of the disease and when you first recognized it as work-related. This information is crucial for processing your claim.
Can I review the information collected about me by the Division?
Yes, you have the right to request information that the Division collects or maintains about you and your workers' compensation claim. Under Texas Government Code, you are entitled to review this information and request corrections if any inaccuracies are found.
Not completing all sections of the DWC Form-041. Each box must be filled out to ensure the claim is processed.
Failing to provide accurate employee information. This includes the correct name, social security number, and contact details.
Incorrectly stating the date of injury. Ensure the date is accurate and matches any other documents related to the claim.
Omitting details about the injury location. Clearly specify where the injury occurred, including county and state.
Not including the supervisor's name or employer's contact information. This information is crucial for communication regarding the claim.
Failing to mention whether the injury is an occupational disease. If applicable, provide details about exposure and related dates.
Not signing the form. The injured employee or representative must sign and date the form for it to be valid.
Submitting the form after the one-year deadline. Claims must be filed within one year of the injury date or knowledge of the work-related condition.
The DWC Form-041 is essential for filing a workers' compensation claim in Texas. However, several other forms and documents are often used in conjunction with it to facilitate the claims process. Understanding these documents can help ensure that all necessary information is submitted accurately and in a timely manner.
By familiarizing oneself with these forms, individuals can navigate the workers' compensation process more effectively. Each document plays a crucial role in ensuring that claims are processed smoothly and that both employees and employers fulfill their obligations under Texas law.
The DWC 041 form is an essential document for filing a claim for workers' compensation in Texas. However, it shares similarities with several other important forms related to workplace injuries and compensation claims. Here’s a breakdown of six documents that are akin to the DWC 041 form:
Understanding these forms can help streamline the process of filing a claim and ensure that all necessary information is provided. Each document plays a vital role in the overall workers' compensation system, supporting both employees and employers in addressing work-related injuries.
When filling out the DWC Form-041 for a workers' compensation claim in Texas, it is essential to follow specific guidelines to ensure accuracy and compliance. Below is a list of things you should and should not do while completing the form.
Understanding the DWC 041 form is essential for anyone filing a claim for workers’ compensation in Texas. However, several misconceptions can lead to confusion. Here are seven common misconceptions and clarifications regarding the DWC 041 form:
This is incorrect. The form must be filed within one year of the date of injury or within one year from when the injured employee knew or should have known the injury was work-related.
While the injured employee is the primary person responsible for filing, a representative can also complete the form on their behalf.
Filing the form does not guarantee benefits. The claim will be reviewed, and eligibility will be determined based on the specifics of the case.
This is not true. The injury must be shown to be caused by work-related activities, and documentation is necessary to establish this connection.
While the DWC 041 form is crucial, additional documentation may be required depending on the specifics of the claim and the employer's insurance requirements.
This is misleading. The injury should be reported to the employer as soon as possible, as this is often a prerequisite for filing the claim.
Currently, the DWC 041 form must be submitted in hard copy. Ensure that you send it to the correct address provided by the Texas Department of Insurance.
When filling out the DWC 041 form for a workers' compensation claim in Texas, there are several important points to keep in mind:
Following these guidelines can help ensure a smoother claims process and increase the likelihood of receiving the benefits you are entitled to.