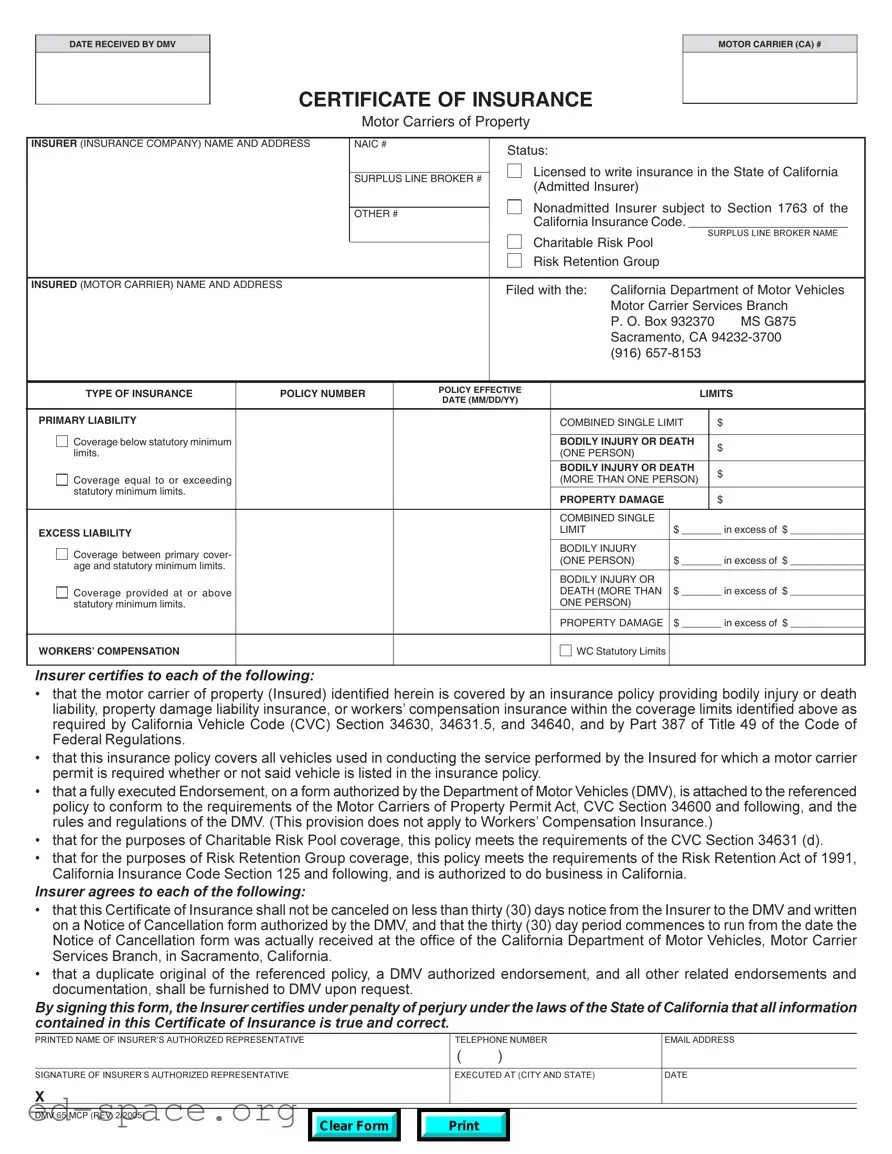
The DMV 65 MCP form plays a crucial role in ensuring that motor carriers of property maintain the necessary insurance coverage as mandated by California law. This form serves as a Certificate of Insurance, confirming that the motor carrier is protected by a valid insurance policy that meets the requirements outlined in the California Vehicle Code and federal regulations. Key details included in the form encompass the name and address of both the motor carrier and the insurer, as well as the policy number, effective dates, and coverage limits. The insurer must certify that the policy covers all vehicles used in the carrier's operations, regardless of whether those vehicles are explicitly listed in the policy. Furthermore, the form stipulates that any cancellation of the insurance must be communicated to the DMV with at least thirty days' notice. This ensures that there is no lapse in coverage, which could jeopardize the carrier's operations. Additionally, specific provisions apply to charitable risk pools and risk retention groups, highlighting the form's comprehensive nature. By signing the DMV 65 MCP, the insurer affirms the accuracy of the information provided, reinforcing the importance of transparency and compliance in the insurance process for motor carriers.
DATE RECEIVED BY DMV
CERTIFICATE OF INSURANCE
Motor Carriers of Property
MOTOR CARRIER (CA) #
INSURER (INSURANCE COMPANY) NAME AND ADDRESS |
NAIC # |
|
Status: |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Licensed to write insurance in the State of California |
|||||
|
|
SURPLUS LINE BROKER # |
||||||||
|
|
(Admitted Insurer) |
|
|
|
|||||
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
Nonadmitted Insurer subject to Section 1763 of the |
|||||
|
|
OTHER # |
|
|||||||
|
|
|
California Insurance Code. ______________________ |
|||||||
|
|
|
|
|
||||||
|
|
|
|
|
Charitable Risk Pool |
SURPLUS LINE BROKER NAME |
||||
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
Risk Retention Group |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
INSURED (MOTOR CARRIER) NAME AND ADDRESS |
|
|
|
Filed with the: |
California Department of Motor Vehicles |
|||||
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Motor Carrier Services Branch |
|||
|
|
|
|
|
|
|
P. O. Box 932370 |
MS G875 |
||
|
|
|
|
|
|
|
Sacramento, CA |
|||
|
|
|
|
|
|
|
(916) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE OF INSURANCE |
POLICY NUMBER |
|
POLICY EFFECTIVE |
|
|
LIMITS |
||||
|
DATE (MM/DD/YY) |
|
|
|||||||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
PRIMARY LIABILITY |
|
|
|
|
|
COMBINED SINGLE LIMIT |
|
$ |
||
|
|
|
|
|
|
|
|
|
|
|
Coverage below statutory minimum |
|
|
|
|
|
BODILY INJURY OR DEATH |
|
$ |
||
limits. |
|
|
|
|
|
(ONE PERSON) |
|
|
||
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
BODILY INJURY OR DEATH |
|
$ |
||
Coverage equal to or exceeding |
|
|
|
|
|
(MORE THAN ONE PERSON) |
|
|||
|
|
|
|
|
|
|
||||
statutory minimum limits. |
|
|
|
|
|
PROPERTY DAMAGE |
|
|
$ |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMBINED SINGLE |
|
|
|
|
EXCESS LIABILITY |
|
|
|
|
|
LIMIT |
|
$ _______ in excess of $ _____________ |
||
|
|
|
|
|
|
|
|
|
|
|
Coverage between primary cover- |
|
|
|
|
|
BODILY INJURY |
|
|
|
|
|
|
|
|
|
(ONE PERSON) |
$ _______ in excess of $ _____________ |
||||
age and statutory minimum limits. |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BODILY INJURY OR |
|
|
|
|
Coverage provided at or above |
|
|
|
|
|
DEATH (MORE THAN |
$ _______ in excess of $ _____________ |
|||
statutory minimum limits. |
|
|
|
|
|
ONE PERSON) |
|
|
|
|
|
|
|
|
|
|
PROPERTY DAMAGE |
$ _______ in excess of $ _____________ |
|||
|
|
|
|
|
|
|
|
|
|
|
WORKERS’ COMPENSATION |
|
|
|
|
|
WC Statutory Limits |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurer certifies to each of the following:
•that the motor carrier of property (Insured) identified herein is covered by an insurance policy providing bodily injury or death liability, property damage liability insurance, or workers’ compensation insurance within the coverage limits identified above as required by California Vehicle Code (CVC) Section 34630, 34631.5, and 34640, and by Part 387 of Title 49 of the Code of Federal Regulations.
•that this insurance policy covers all vehicles used in conducting the service performed by the Insured for which a motor carrier permit is required whether or not said vehicle is listed in the insurance policy.
•that a fully executed Endorsement, on a form authorized by the Department of Motor Vehicles (DMV), is attached to the referenced policy to conform to the requirements of the Motor Carriers of Property Permit Act, CVC Section 34600 and following, and the rules and regulations of the DMV. (This provision does not apply to Workers’ Compensation Insurance.)
•that for the purposes of Charitable Risk Pool coverage, this policy meets the requirements of the CVC Section 34631 (d).
•that for the purposes of Risk Retention Group coverage, this policy meets the requirements of the Risk Retention Act of 1991, California Insurance Code Section 125 and following, and is authorized to do business in California.
Insurer agrees to each of the following:
•that this Certificate of Insurance shall not be canceled on less than thirty (30) days notice from the Insurer to the DMV and written on a Notice of Cancellation form authorized by the DMV, and that the thirty (30) day period commences to run from the date the Notice of Cancellation form was actually received at the office of the California Department of Motor Vehicles, Motor Carrier Services Branch, in Sacramento, California.
•that a duplicate original of the referenced policy, a DMV authorized endorsement, and all other related endorsements and documentation, shall be furnished to DMV upon request.
By signing this form, the Insurer certifies under penalty of perjury under the laws of the State of California that all information contained in this Certificate of Insurance is true and correct.
PRINTED NAME OF INSURER’S AUTHORIZED REPRESENTATIVE |
|
|
|
TELEPHONE NUMBER |
EMAIL ADDRESS |
||
|
|
( |
) |
|
|
||
|
|
|
|
|
|
|
|
SIGNATURE OF INSURER’S AUTHORIZED REPRESENTATIVE |
|
|
|
EXECUTED AT (CITY AND STATE) |
DATE |
||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DMV 65 MCP (REV. 2/2005) |
|
|
|
|
|
|
|
Clear Form
| Fact Name | Description |
|---|---|
| Purpose of the Form | The DMV 65 MCP form serves as a Certificate of Insurance for motor carriers of property in California. |
| Governing Laws | This form is governed by California Vehicle Code Sections 34630, 34631.5, and 34640, as well as Part 387 of Title 49 of the Code of Federal Regulations. |
| Insurance Coverage | The form certifies that the motor carrier is covered by necessary insurance policies, including bodily injury, property damage, and workers’ compensation. |
| Cancellation Notice | The insurer must provide a 30-day notice to the DMV before canceling the insurance, ensuring continued coverage for the motor carrier. |
| Endorsements Requirement | An authorized endorsement must be attached to the policy to meet DMV requirements, ensuring compliance with the Motor Carriers of Property Permit Act. |
| Verification of Information | By signing the form, the insurer certifies that all information provided is true and correct under penalty of perjury. |
Filling out the DMV 65 MCP form is an important step for motor carriers in California to ensure compliance with insurance requirements. After completing the form, it will need to be submitted to the California Department of Motor Vehicles for processing.
What is the DMV 65 MCP form?
The DMV 65 MCP form is a Certificate of Insurance specifically for Motor Carriers of Property in California. It is required to demonstrate that a motor carrier has the necessary insurance coverage as mandated by California law. This form must be filed with the California Department of Motor Vehicles (DMV) to ensure compliance with state regulations regarding commercial vehicle operations.
Who needs to file the DMV 65 MCP form?
Any motor carrier operating in California that requires a motor carrier permit must file the DMV 65 MCP form. This includes businesses that transport goods for hire. The form confirms that the carrier has adequate insurance coverage for bodily injury, property damage, and workers' compensation, as required by law.
What information is required on the DMV 65 MCP form?
The form requires detailed information about the motor carrier, including the name and address of the insured, the insurance company, policy number, and coverage limits. It also asks for the type of insurance being provided, such as primary liability or workers' compensation, and must include a certification from the insurer regarding the coverage's compliance with California Vehicle Code requirements.
How does one submit the DMV 65 MCP form?
The DMV 65 MCP form can be submitted by mailing it to the California Department of Motor Vehicles, Motor Carrier Services Branch. The mailing address is P.O. Box 932370, MS G875, Sacramento, CA 94232-3700. It is important to ensure that the form is complete and accurate to avoid delays in processing.
What happens if the insurance policy changes or is canceled?
If the insurance policy changes or is canceled, the insurer must notify the DMV at least thirty days in advance. This notification must be made using a Notice of Cancellation form authorized by the DMV. It is crucial to maintain continuous coverage to avoid penalties or disruptions in the motor carrier's operations.
Can the DMV 65 MCP form be filed electronically?
Missing Information: Failing to fill in all required fields can lead to delays. Ensure every section is complete, including the motor carrier name and address.
Incorrect Dates: Entering the wrong policy effective date can cause issues. Always double-check that the date is in the correct format (MM/DD/YY).
Policy Limits Errors: Providing incorrect limits for bodily injury or property damage can result in rejection. Make sure the limits meet California's statutory minimums.
Omitting the Endorsement: Not attaching the required endorsement can invalidate the form. Confirm that the endorsement is included and properly executed.
Inaccurate Insurance Company Information: Listing incorrect details about the insurer can lead to complications. Verify the insurer's name, address, and NAIC number.
Signature Issues: Forgetting to sign the form or having an unauthorized person sign can cause problems. Ensure the authorized representative signs and dates the document.
Not Notifying DMV of Cancellations: Failing to provide a 30-day notice for policy cancellations can lead to penalties. Always send the notice as required.
Ignoring Coverage Requirements: Not meeting the specific coverage requirements for workers' compensation or other policies can result in rejection. Review the necessary coverage types carefully.
Submitting Without a Copy: Not including a duplicate original of the insurance policy can delay processing. Keep a copy for your records and provide one to the DMV as needed.
The DMV 65 MCP form is a crucial document for motor carriers in California, serving as a Certificate of Insurance. Along with this form, several other documents are often required to ensure compliance with state regulations. Below is a list of related forms and documents that are commonly used in conjunction with the DMV 65 MCP form.
These documents collectively help ensure that motor carriers meet the necessary legal requirements for operation in California. Properly managing these forms can prevent potential legal issues and ensure smooth business operations.
The DMV 65 MCP form is a critical document for motor carriers in California, primarily serving as a Certificate of Insurance. Several other documents share similarities with this form in terms of purpose and requirements. Here are seven such documents:
When filling out the DMV 65 MCP form, it's essential to be thorough and accurate. Here’s a helpful list of things you should and shouldn't do to ensure a smooth process.
By following these guidelines, you can help ensure that your DMV 65 MCP form is processed efficiently. Taking the time to carefully complete the form can save you from potential headaches down the line.
This form is required for any motor carrier of property operating in California, regardless of the size of the business. Even small operators must comply with this requirement.
Changes in insurance coverage or company details necessitate an update to the DMV 65 MCP form. Keeping it current is essential to remain compliant.
The form certifies that all vehicles used by the motor carrier are covered under the insurance policy, even if they are not listed specifically in the policy.
This form also pertains to workers' compensation insurance, ensuring that all necessary coverage types are addressed for motor carriers.
While the insurer must provide 30 days' notice before cancellation, it does not guarantee that the policy will remain active indefinitely.
The insurance company must be licensed to write insurance in California and comply with specific regulations to issue this form.
The DMV has the authority to verify the accuracy of the information submitted. Any discrepancies can lead to penalties or the denial of permits.
Here are key takeaways for filling out and using the DMV 65 MCP form: