When individuals or families navigate the complexities of accessing and managing military medical records, one crucial tool at their disposal is the DD 2870 form. This form fundamentally serves as an authorization for the disclosure of information, playing a pivotal role in ensuring that military personnel and their dependents can grant consent for the release of their medical or dental records to requested parties. The essence of the DD 2870 form lies in its ability to bridge the privacy of patients with the necessity of sharing medical information under specific circumstances, such as for continuing healthcare, processing insurance claims, or even facilitating medical board proceedings. By properly completing and submitting this form, service members take an important step towards managing their healthcare more effectively, maintaining control over who has access to their sensitive medical information. Understanding the appropriate way to fill out and use the form unlocks the potential for a smoother interaction with healthcare providers and administrative processes, making it a critical aspect of healthcare management within the military community.
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
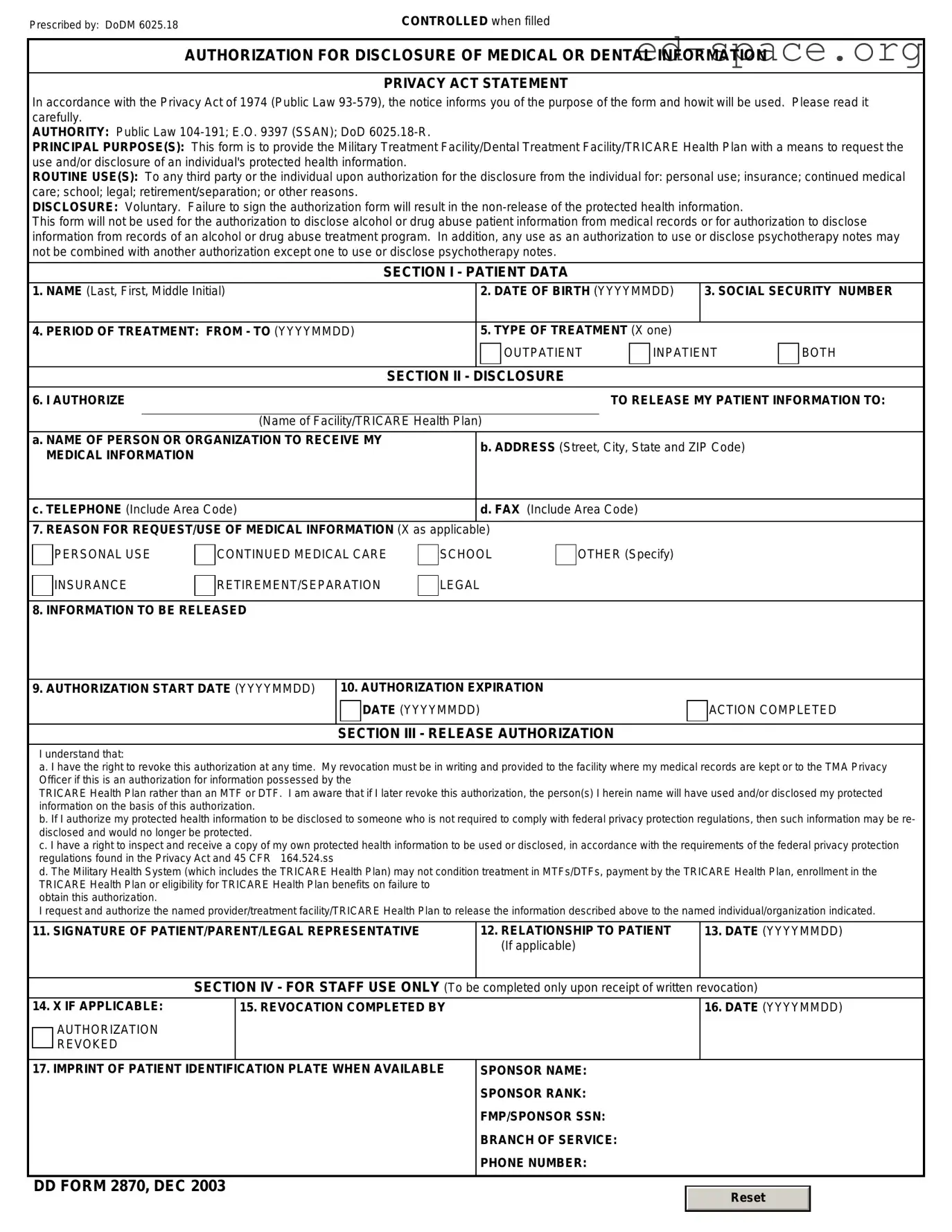
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
| Fact Number | Description |
|---|---|
| 1 | The DD 2870 form is titled Authorization for Disclosure of Medical or Dental Information. |
| 2 | It is used by military members, veterans, and their dependents to authorize the release of medical or dental information by military health care providers. |
| 3 | The form allows individuals to specify which information can be disclosed, including the date range of the medical records to be released. |
| 4 | Filling out the DD 2870 properly is necessary to ensure that only authorized parties receive sensitive health information. |
| 5 | The form requires the identification of the individual whose records are to be disclosed, the organization receiving the disclosure, and the purpose of the disclosure. |
| 6 | A signature from the patient or their legal representative, along with the date, is mandatory to validate the authorization. |
| 7 | There are no state-specific versions of the DD 2870 form as it is a federal document used across the United States within the Department of Defense. |
| 8 | Once completed, the form should be submitted to the appropriate medical facility's records department or the designated point of contact. |
Upon deciding to fill out the DD 2870 form, it's crucial to approach the task with attention to detail. This document plays a pivotal role in ensuring that the designated processes are conducted smoothly, enabling all involved parties to proceed with clarity and understanding. The completion of this form, therefore, must be approached methodically, ensuring all data provided is accurate and comprehensive. Below are the steps designed to guide individuals through the process, ensuring a thorough and correct submission.
Following submission, it is advisable to keep a copy of the completed form and any confirmations of receipt for personal records. This ensures that one has evidence of the submission and can follow up appropriately, should there be any inquiries or need for further action. The process of filling out and submitting the DD 2870 form, while meticulous, is a crucial step in facilitating the intended administrative or operational actions, and as such, warrants careful attention to each detail.
What is a DD 2870 form?
The DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, is a document used by military personnel and their dependents. It grants permission for the release of specific health information to designated individuals, organizations, or agencies. This form is often used to share medical records between healthcare providers or to allow access to medical information for specific purposes such as insurance claims or medical care coordination.
How do I complete the DD 2870 form?
To complete the DD 2870 form, you must provide personal identification information, including the full name of the patient, their date of birth, and the last four digits of their Social Security Number or Military ID. You must also specify the information to be disclosed, the purpose of the disclosure, and to whom the information will be released. It's essential to indicate the format in which you wish to receive the information (e.g., paper copy, digital format) and to acknowledge the consent expiration date. Finally, the patient or their legal representative must sign and date the form, indicating their authorization for the release of the specified medical or dental information.
Who needs to sign the DD 2870 form?
The DD 2870 form must be signed by the individual whose medical or dental information is to be disclosed, affirming their consent for the release. If the individual is a minor or is not capable of signing the form due to medical reasons, a parent, legal guardian, or a legally authorized representative may sign on their behalf. The signature is a requirement to validate the authorization for disclosure and without it, the request for information release cannot be processed.
Where do I submit the completed DD 2870 form?
The completed DD 2870 form should be submitted to the healthcare facility where the medical or dental records are held. Each facility may have its specific submission guidelines or office designated for handling these forms. It is advisable to contact the healthcare provider's records department or patient administration department to confirm the correct submission process and address. Some facilities may allow submission via mail, fax, or secure electronic methods, depending on their policies and the sensitivity of the information being disclosed.
When individuals set out to fill the DD 2870 form, which is used to request medical or dental records from military facilities, several common mistakes can occur. These errors can lead to delays in the processing of requests, or in some cases, the denial of the request altogether. It's important to approach this document with care to ensure all the necessary information is correctly provided. Here is an expanded list of six common mistakes made:
Not verifying eligibility before submission: Many individuals assume they are automatically eligible to receive records without first verifying their eligibility. This mistake can lead to the rejection of their request.
Incorrect or incomplete personal information: It’s crucial to double-check that all personal information, including full name, social security number, and date of birth, is correct and fully filled out. Misinformation or incomplete fields can prevent the request from being processed.
Failing to specify the records needed: The DD 2870 form requires the requester to specify which medical or dental records are needed. A common mistake is not being specific enough about the records required, leading to incomplete fulfillment of the request.
Omitting the purpose of the request: The form asks for the reason for the records request. Neglecting to state the purpose can cause delays, as officials may need to clarify the intention behind the request before processing.
Not including the correct mailing address: If the requester fails to provide a correct and complete mailing address where the records should be sent, it can result in the records being sent to the wrong place or not being sent at all.
Forgetting to sign and date the form: One of the simplest yet most frequently made mistakes is not signing or dating the form. A signature is required to validate the request, and without it, the process cannot proceed.
Avoiding these mistakes can significantly streamline the process of obtaining medical or dental records through the DD 2870 form. Ensuring all information is accurate and complete before submission is key to a successful request.
When you're navigating the maze of paperwork and forms required for various legal, medical, and governmental processes, understanding the context and companions of each form can significantly ease your journey. The DD Form 2870, or "Authorization for Disclosure of Medical or Dental Information," is frequently utilized within the military sector to authorize the release of health information. However, it is often accompanied by other documentation, each serving its unique purpose in ensuring that all necessary information is accurately communicated and legally documented. Understanding these companion documents can help streamline the process and ensure no detail is overlooked.
The intricate interplay between the DD 2870 and its often-required accompanying documents underscores the importance of a thorough preparation process. Whether you're a service member, a veteran, or acting on behalf of one, understanding these additional documents ensures a smoother navigation through the procedural aspects of accessing medical and dental information. While the specific requirements may vary based on the situation and jurisdiction, being prepared with a comprehensive set of documents will facilitate a more efficient and secure information disclosure process.
Health Insurance Portability and Accountability Act (HIPAA) Authorization Form: Similar to the DD 2870 form, the HIPAA Authorization Form is used to authorize the release of an individual's health information. Both documents require specific details about the individual whose information is being disclosed, the nature of the information to be released, and the purpose of the disclosure. They ensure that personal health information is shared securely and in compliance with federal privacy laws.
Medical Records Release Form: This form, like the DD 2870, permits healthcare providers to share a patient's medical records with specified individuals or organizations. The primary similarity lies in their function to facilitate the transfer of protected health information, contingent upon the patient's consent. Both forms delineate the scope and limitations of the information to be disclosed.
Power of Attorney for Health Care: While the Power of Attorney for Health Care primarily designates an individual to make healthcare decisions on behalf of someone else, it is similar to the DD 2870 in that it involves granting permissions related to personal health information. Both documents play vital roles in ensuring a person's health care preferences are honored and that trusted parties can access necessary information for decision-making.
General Consent Form for Medical Treatment: This form shares its purpose with the DD 2870 in the context of granting permission, albeit more broadly for medical treatment rather than the release of medical records. They are both integral to the medical process, ensuring that patients or their representatives agree to specific actions concerning their health care.
Privacy Act Release Form: Much like the DD 2870, this document is used to authorize the disclosure of personal information, but under the provisions of the Privacy Act. Both forms require clear consent from the individual for their information to be shared, highlighting the individual's control over their personal data.
Consent to Release Financial Information Form: Although this form focuses on financial rather than health information, it parallels the DD 2870 in its function to authorize the sharing of private data. Each document mandates explicit permission from the individual for certain information to be disclosed to designated parties.
Authorization for Release of Employment Information Form: This form is akin to the DD 2870 in that it permits the disclosure of an individual's employment-related details. Both forms facilitate the exchange of sensitive information, emphasizing the necessity for the individual's consent and defining the scope of the disclosure.
The DD Form 2870, also known as the Authorization for Disclosure of Medical or Dental Information, is a document used within the Department of Defense. It is filled out when an individual wishes to allow the release of their medical or dental records to a designated person or entity. Handling this form properly ensures that personal health information is shared respectfully and securely. Here are six dos and don'ts to consider when completing the DD 2870 form.
Things You Should Do:
Read the instructions carefully before you start filling out the form to ensure you understand the requirements and the type of information needed.
Use black ink and write legibly to ensure that all information is clear and understandable, minimizing the risk of errors or delays.
Verify that you have the correct version of the form, as outdated forms may not be accepted and could lead to the rejection of your request.
Include all necessary details, such as your full name, date of birth, social security number, and the specific records you are requesting to be released.
Sign and date the form in the designated area to provide the required authorization for the release of your medical or dental records.
Keep a copy of the completed form for your records, as this will help you track the request and address any issues that may arise.
Things You Shouldn't Do:
Do not leave any required fields empty. Incomplete forms might delay or prevent the processing of your request.
Do not forget to specify the purpose of the disclosure. Vague descriptions can lead to confusion and potential misuse of your information.
Avoid using pencil or colors of ink other than black, as this can cause issues with scanning or photocopying the form.
Do not guess information; if you are unsure about a detail, verify it before completing the form to avoid inaccuracies.
Refrain from providing more information than what is requested. Over-disclosing can lead to unnecessary exposure of personal health information.
Do not forget to review the form for errors or omissions before submitting it. Mistakes could lead to delays or rejection of your authorization request.
The DD 2870 form is often surrounded by misconceptions that can lead to confusion. To ensure clarity, let's address some of these misunderstandings directly.
It's available for non-military use: The DD 2870 form is specifically designed for military members, their families, and retirees to request the release of medical or dental information. It is not intended for use by the general public.
It covers all medical records automatically: Completing a DD 2870 form does not grant access to all medical records by default. The form requires specification of the types of records needed, and only those authorized will be released.
Parental consent isn't required for minors: For dependents under the age of 18, parental or legal guardian consent is necessary when requesting medical information via the DD 2870 form.
Signing the form waives all HIPAA protections: Filling out and signing the DD 2870 does not waive all HIPAA protections. It authorizes the release of specific information to individuals or organizations named in the form, in accordance with HIPAA regulations.
There is a filing fee: There is no fee to submit a DD 2870 form. The process of requesting medical records through this form is free of charge for eligible individuals.
Electronic signatures are not accepted: Depending on the institution and its capabilities, electronic signatures on a DD 2870 form can be accepted. It's essential to confirm with the specific medical records department.
Any healthcare provider can sign off on requests: Only the healthcare provider who is either primarily responsible for the patient’s care or is the head of the department that maintains the records can legally endorse requests made on the DD 2870 form.
The form offers instant access to records: Submitting a DD 2870 form does not guarantee immediate access to medical records. The processing time can vary depending on the facility’s policy, the volume of requests, and the specific information being requested.
Understanding these key points can alleviate common concerns and misconceptions regarding the DD 2870 form, ensuring smoother interactions and processes for those who need to use it.
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," serves as a critical tool for individuals seeking to grant permission for the release of their health information. Understanding how to properly fill out and use this form ensures individuals maintain control over their personal health information while complying with legal standards. The process may seem daunting initially, but grasping a few key takeaways can simplify it significantly.
By understanding and following these key takeaways, individuals can navigate the complexities of sharing their health information with confidence, ensuring that their privacy is protected while allowing necessary access to their medical or dental records.
Illinois Wage Verification Form - It serves as a formal request for income verification from employers.
Form 2790 Self Employment Record - Information recorded on the form must be truthful and reflect actual financial activities.