The DB 450 Disability form is an essential document for individuals seeking disability benefits in New York State. Designed to streamline the claims process, this form requires claimants to provide detailed personal information, including their name, address, and Social Security number. Claimants must describe the nature of their disability, including when it occurred and whether they have recovered. Additionally, the form asks about employment history and any wages received during the disability period. Part A focuses on the claimant's information, while Part B is dedicated to the health care provider’s assessment, which must be filled out completely to avoid delays. Health care providers need to offer insights into the diagnosis, treatment dates, and the claimant's ability to work. Completing the DB 450 accurately and promptly is crucial, as it directly impacts the processing of claims for disability benefits. The instructions on the form guide users on how to submit it correctly, ensuring that all necessary information is included to facilitate a smooth claims experience.
New York State |
|
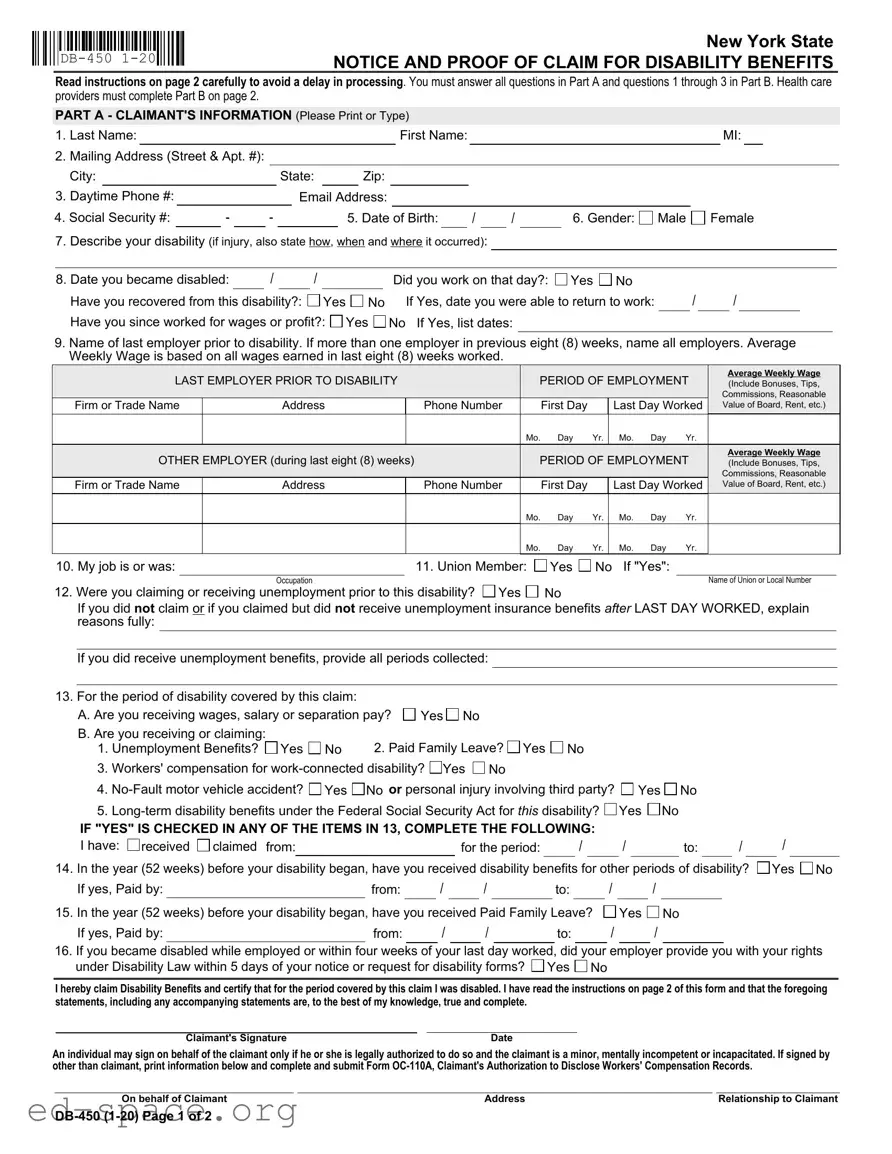
NOTICE AND PROOF OF CLAIM FOR DISABILITY BENEFITS |
Read instructions on page 2 carefully to avoid a delay in processing. You must answer all questions in Part A and questions 1 through 3 in Part B. Health care providers must complete Part B on page 2.
PART A - CLAIMANT'S INFORMATION (Please Print or Type)
1. |
Last Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name: |
|
|
|
|
|
|
|
MI: |
|
|
|||
2. |
Mailing Address (Street & Apt. #): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
City: |
|
|
|
|
|
|
State: |
|
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
||||||
3. Daytime Phone #: |
|
|
|
|
|
|
Email Address: |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
4. Social Security #: |
|
- |
|
- |
|
|
|
5. Date of Birth: |
|
|
/ |
|
/ |
|
6. Gender: |
Male |
Female |
|
||||||||||
7.Describe your disability (if injury, also state how, when and where it occurred):
8. Date you became disabled: |
|
/ |
|
/ |
|
|
|
Did you work on that day?: Yes No |
/ |
/ |
|
|
||
Have you recovered from this disability?: |
|
Yes |
No |
If Yes, date you were able to return to work: |
|
|
||||||||
Have you since worked for wages or profit?: |
Yes |
No If Yes, list dates: |
|
|
|
|
|
|
||||||
9.Name of last employer prior to disability. If more than one employer in previous eight (8) weeks, name all employers. Average Weekly Wage is based on all wages earned in last eight (8) weeks worked.
LAST EMPLOYER PRIOR TO DISABILITY |
|
PERIOD OF EMPLOYMENT |
Average Weekly Wage |
|||||||
|
(Include Bonuses, Tips, |
|||||||||
|
|
|
|
|
|
|
|
|
|
Commissions, Reasonable |
Firm or Trade Name |
Address |
|
Phone Number |
|
First Day |
|
Last Day Worked |
Value of Board, Rent, etc.) |
||
|
|
|
|
Mo. |
Day |
Yr. |
Mo. |
Day |
Yr. |
|
OTHER EMPLOYER (during last eight (8) weeks) |
|
PERIOD OF EMPLOYMENT |
Average Weekly Wage |
|||||||
|
(Include Bonuses, Tips, |
|||||||||
|
|
|
|
|
|
|
|
|
|
Commissions, Reasonable |
Firm or Trade Name |
Address |
|
Phone Number |
|
First Day |
|
Last Day Worked |
Value of Board, Rent, etc.) |
||
|
|
|
|
Mo. |
Day |
Yr. |
Mo. |
Day |
Yr. |
|
|
|
|
|
Mo. |
Day |
Yr. |
Mo. |
Day |
Yr. |
|
10. My job is or was: |
|
11. Union Member: |
Yes |
No If "Yes": |
||
|
Occupation |
|
|
|
|
Name of Union or Local Number |
12. Were you claiming or receiving unemployment prior to this disability? |
Yes |
No |
|
|
||
If you did not claim or if you claimed but did not receive unemployment insurance benefits after LAST DAY WORKED, explain reasons fully:
If you did receive unemployment benefits, provide all periods collected:
13. For the period of disability covered by this claim: |
|
|
|
A. Are you receiving wages, salary or separation pay? |
Yes No |
||
B. Are you receiving or claiming: |
|
2. Paid Family Leave? Yes No |
|
1. Unemployment Benefits? |
Yes No |
||
3.Workers' compensation for
4.
5.
IF "YES" IS CHECKED IN ANY OF THE ITEMS IN 13, COMPLETE THE FOLLOWING:
I have: |
received |
claimed from: |
|
for the period: |
|
/ |
|
/ |
|
to: |
|
/ |
14. In the year (52 weeks) before your disability began, have you received disability benefits for other periods of disability?
If yes, Paid by: |
|
from: |
|
/ |
|
/ |
|
to: |
|
/ |
|
/ |
/
Yes No
15. In the year (52 weeks) before your disability began, have you received Paid Family Leave?
If yes, Paid by: |
from: |
/ |
/ |
to: |
Yes
/
No
/
16.If you became disabled while employed or within four weeks of your last day worked, did your employer provide you with your rights under Disability Law within 5 days of your notice or request for disability forms? Yes No
I hereby claim Disability Benefits and certify that for the period covered by this claim I was disabled. I have read the instructions on page 2 of this form and that the foregoing statements, including any accompanying statements are, to the best of my knowledge, true and complete.
Claimant's Signature |
Date |
An individual may sign on behalf of the claimant only if he or she is legally authorized to do so and the claimant is a minor, mentally incompetent or incapacitated. If signed by other than claimant, print information below and complete and submit Form
On behalf of Claimant |
Address |
Relationship to Claimant |
PART B - HEALTH CARE PROVIDER'S STATEMENT (Please Print or Type)
THE HEALTH CARE PROVIDER'S STATEMENT MUST BE FILLED IN COMPLETELY. THE ATTENDING HEALTH CARE PROVIDER SHALL COMPLETE AND RETURN TO THE CLAIMANT WITHIN SEVEN (7) DAYS OF RECEIPT OF THIS FORM. For item
1. Last Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MI: |
|
|
||||||||||
2.Gender: |
Male |
Female |
|
3. Date of Birth: |
/ |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
4. Diagnosis/Analysis: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diagnosis Code: |
|
|
|
|
|
|
|
|
|
|||||||||||
|
a. Claimant's symptoms: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
b. Objective findings: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. Claimant hospitalized?: |
Yes |
No |
From: |
|
|
|
/ |
|
|
/ |
|
|
To: |
|
|
/ |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
6. Operation indicated?: |
Yes |
No |
a. Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Date |
/ |
|
/ |
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
ENTER DATES FOR THE FOLLOWING |
|
|
|
|
|
|
|
|
|
|
MONTH |
|
|
|
|
|
|
DAY |
|
|
|
|
YEAR |
|
||||||||||||||||||||
a Date of your first treatment for this disability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
b.Date of your most recent treatment for this disability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
c. Date Claimant was unable to work because of this disability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
d.Date Claimant will again be able to perform work (Even if considerable question |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
exists, estimate date. Avoid use of terms such as unknown or undetermined.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
e.If pregnancy related, please check box and enter the date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
estimated delivery date OR |
actual delivery date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
8. In your opinion, is this disability the result of injury arising out of and in the course of employment or occupational disease?:
|
Yes |
No If "Yes", has Form |
Yes |
No |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
I certify that I am a: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
(Physician, Chiropractor, Dentist, Podiatrist, Psychologist, |
Licensed or Certified in the State of |
|
|
License Number |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Health Care Provider's Printed Name |
|
|
Health Care Provider's Signature |
|
|
|
Date |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Health Care Provider's Address |
|
|
|
|
|
|
|
Phone # |
|||||||
IMPORTANT NOTICE TO CLAIMANT - READ THESE INSTRUCTIONS CAREFULLY
PLEASE NOTE: Do not date and file this form prior to your first date of disability. In order for your claim to be processed, Parts A and B must be completed.
1.If you are using this form because you became disabled while employed or you became disabled within four (4) weeks after termination of employment, your completed claim should be mailed within thirty (30) days of your first date of disability to your employer or your last employer's insurance carrier. You may find your employer's disability insurance carrier on the Workers' Compensation Board's website, www.wcb.ny.gov, using Employer Coverage Search.
2.If you are using this form because you became disabled after having been unemployed for more than four (4) weeks, your completed claim MUST be mailed to: Workers' Compensation Board, Disability Benefits Bureau, PO Box 9029, Endicott, NY
If you do not receive a response within 45 days or if you have questions about your disability benefits claim, please call your employer's insurance carrier. For general information about disability benefits, please visit www.wcb.ny.gov or call the Board's Disability Benefits Bureau at (877)
Notification Pursuant to the New York Personal Privacy Protection Law (Public Officers Law Article
HIPAA NOTICE - In order to adjudicate a workers' compensation claim or disability benefits claim, WCL
Disclosure of Information: The Board will not disclose any information about your case to any unauthorized party without your consent. If you choose to have such information disclosed to an unauthorized part, you must file with the Board an original signed Form
An employer or insurer, or any employee, agent, or person acting on behalf of an employer or insurer, who KNOWINGLY MAKES A FALSE STATEMENT OR REPRESENTATION as to a material fact in the course of reporting, investigation of, or adjusting a claim for any benefit or payment under this chapter for the purpose of avoiding provision of such payment or benefit SHALL BE GUILTY OF A CRIME AND SUBJECT TO SUBSTANTIAL FINES AND IMPRISONMENT.
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The DB-450 form is used to file a claim for disability benefits in New York State. |
| Claimant Information | Part A requires the claimant's personal details, including name, address, and social security number. |
| Health Care Provider | Part B must be completed by a health care provider who treats the claimant for their disability. |
| Submission Timeline | Claims should be submitted within 30 days of the first date of disability to avoid delays. |
| Governing Law | The DB-450 form is governed by New York Workers' Compensation Law. |
| Eligibility Requirements | Claimants must provide proof of their disability and may need to show employment history. |
| Signature Requirement | The claimant must sign the form, certifying that the information is true and complete. |
| Incomplete Submissions | Failure to complete all required sections may delay the processing of the claim. |
| Privacy Notice | The form includes a privacy notice regarding the handling of personal information. |
| Contact Information | For questions, claimants can contact the Workers' Compensation Board at (877) 632-4996. |
Completing the DB-450 Disability form is an essential step in filing a claim for disability benefits. This process requires attention to detail and accurate information to ensure timely processing. Below are the steps to guide you through filling out the form effectively.
Once the form is submitted, the next steps involve waiting for processing. You may receive a response within 45 days, or you can reach out to your employer's insurance carrier for updates. Understanding this process can help alleviate some of the stress associated with filing for disability benefits.
What is the DB 450 Disability form?
The DB 450 Disability form is a claim form used in New York State to apply for disability benefits. It serves as a notice and proof of claim for individuals who have become disabled and are seeking financial assistance during their recovery period.
Who needs to fill out the DB 450 form?
Both the claimant and their healthcare provider must complete the form. The claimant provides personal information and details about their disability, while the healthcare provider fills out their section to verify the disability and provide medical information.
What information is required from the claimant?
The claimant must provide personal details such as their name, address, phone number, Social Security number, date of birth, and gender. Additionally, they must describe their disability, including when and how it occurred, and provide information about their employment history and any other benefits they may be receiving.
How should the form be submitted?
The completed form should be mailed to the claimant's employer or the employer's insurance carrier if the disability occurred while employed or within four weeks after leaving a job. If the claimant has been unemployed for over four weeks, the form should be sent to the Workers' Compensation Board's Disability Benefits Bureau.
What happens if the form is incomplete?
If the form is incomplete, it may delay the processing of the claim. It is essential to answer all questions fully and accurately to avoid any issues with benefit payments.
How long does it take to process the claim?
The processing time can vary, but claimants should expect a response within 45 days. If there are any questions or concerns, it is advisable to contact the employer's insurance carrier for updates on the claim status.
Can the claimant authorize someone else to sign the form?
Yes, an individual may sign on behalf of the claimant if they are legally authorized to do so. This is typically applicable for minors or individuals who are mentally incompetent or incapacitated.
What if the claimant has received disability benefits in the past?
The claimant must disclose any previous disability benefits received in the year before the current claim. This information is crucial for determining eligibility and the amount of benefits that may be awarded.
Is it necessary for the healthcare provider to fill out their section promptly?
Yes, the healthcare provider must complete their section and return it to the claimant within seven days of receiving the form. Timely submission helps ensure that the claim is processed without unnecessary delays.
What should the claimant do if they have questions about the form?
If the claimant has questions about the DB 450 form or the disability benefits process, they can visit the Workers' Compensation Board's website or call the Disability Benefits Bureau for assistance.
Incomplete Information: Many individuals fail to provide all necessary details in Part A. Missing information, such as the Social Security number or mailing address, can lead to delays in processing the claim.
Not Following Instructions: Ignoring the instructions on page 2 can create problems. Each section must be completed as directed to ensure a smooth processing experience.
Incorrect Dates: People often make mistakes when entering dates, particularly the date of disability onset. Providing accurate dates is crucial for determining eligibility.
Missing Employer Information: If you had multiple employers in the eight weeks before your disability, it’s important to list all of them. Omitting any employer can result in an inaccurate assessment of your claim.
Failure to Sign: Some claimants forget to sign the form. A missing signature invalidates the claim, causing further delays.
Neglecting to Include Health Care Provider’s Statement: The health care provider must complete Part B. If this section is not filled out completely, it can hinder the approval of benefits.
The DB 450 Disability form is essential for filing a claim for disability benefits in New York State. However, there are additional forms and documents that may be required to support your claim. Below is a list of these documents, along with brief descriptions of each.
Having these documents ready can streamline the claims process and reduce the likelihood of delays. Ensure that all information is accurate and complete to support your claim effectively.
When filling out the DB-450 Disability form, it’s essential to be thorough and accurate. Here’s a helpful list of things to do and avoid to ensure your claim is processed smoothly.
By keeping these points in mind, you can navigate the process more effectively and increase the likelihood of a successful claim.
Understanding the DB-450 Disability form is crucial for anyone seeking disability benefits in New York State. However, several misconceptions can lead to confusion and delays in processing claims. Below are four common misconceptions explained.
Many individuals believe they can skip certain sections of the DB-450 form. In reality, all questions in Part A and specific questions in Part B must be answered completely. Incomplete forms can result in delays in processing your claim.
Some claimants think that Part B of the form, which is the Health Care Provider's Statement, is solely the responsibility of their healthcare provider. While it is true that a healthcare provider must complete this section, claimants also have a role in ensuring that their provider submits the form within the required timeframe.
There is a belief that submitting the DB-450 form late will not impact the claim. However, if the form is not mailed within 30 days of the first date of disability, it may lead to a denial of benefits. Timeliness is essential in the claims process.
Many people assume that providing their Social Security number is mandatory. While it is requested for identification purposes, it is voluntary. Not providing it will not lead to a denial of your claim or a reduction in benefits.