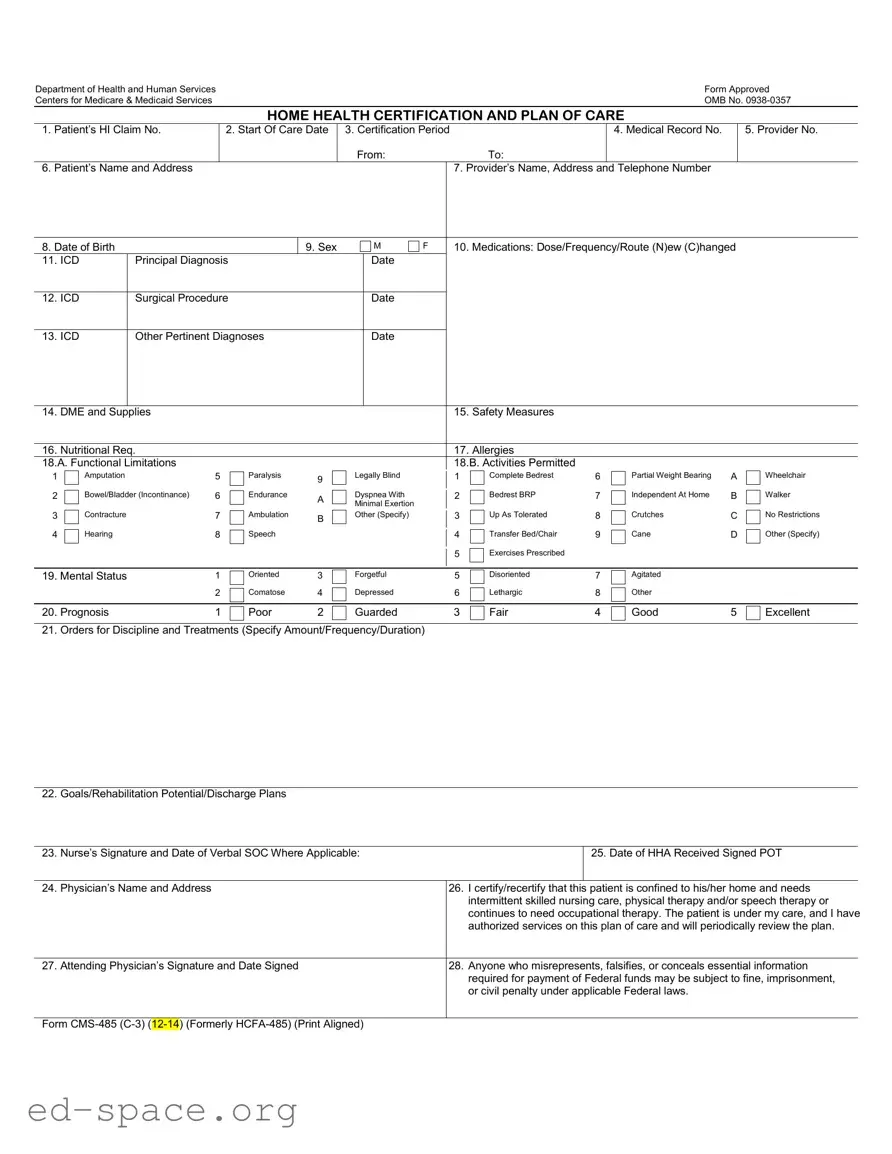
The CMS 485 form, officially known as the Home Health Certification and Plan of Care, plays a crucial role in the provision of home health services under Medicare. This form is essential for documenting a patient's need for skilled nursing care, physical therapy, or other therapeutic services. It encompasses various important sections, including patient identification details, the certification period, and the provider's information. Additionally, it requires a comprehensive assessment of the patient's medical condition, including principal diagnoses and any pertinent surgical procedures. The form also addresses the patient's functional limitations and mental status, allowing healthcare providers to outline specific goals for rehabilitation and discharge plans. Furthermore, it includes critical information regarding medications, allergies, and necessary medical equipment or supplies. The attending physician must certify the patient's eligibility for home health services, ensuring that the information provided is accurate and complete. This certification is vital not only for patient care but also for compliance with federal regulations, as any misrepresentation could lead to serious legal consequences. Understanding the intricacies of the CMS 485 form is essential for healthcare providers to facilitate effective patient care and navigate the complexities of Medicare reimbursement.
Department of Health and Human Services |
Form Approved |
Centers for Medicare & Medicaid Services |
OMB No. |
HOME HEALTH CERTIFICATION AND PLAN OF CARE
1. |
Patient’s HI Claim No. |
2. Start Of Care Date |
3. Certification Period |
|
4. Medical Record No. |
5. Provider No. |
|
|
|
From: |
To: |
|
|
6. |
Patient’s Name and Address |
|
|
7. Provider’s Name, Address and Telephone Number |
|
|
8. Date of Birth |
|
9. Sex |
M |
F |
10. Medications: Dose/Frequency/Route (N)ew (C)hanged |
11. ICD |
Principal Diagnosis |
|
Date |
|
|
|
|
|
|
|
|
12. ICD |
Surgical Procedure |
|
Date |
|
|
|
|
|
|
|
|
13. ICD |
Other Pertinent Diagnoses |
|
Date |
|
|
|
|
|
|
|
|
14. |
DME and Supplies |
15. |
Safety Measures |
|
|
|
|
16. |
Nutritional Req. |
17. |
Allergies |
18.A. Functional Limitations |
18.B. Activities Permitted |
||
1
2
3
4
Amputation |
5 |
|
Paralysis |
9 |
|
|
|
|
|
Bowel/Bladder (Incontinance) |
6 |
|
Endurance |
A |
|
||||
|
|
|
|
|
Contracture |
7 |
|
Ambulation |
B |
|
||||
|
|
|
|
|
Hearing |
8 |
|
Speech |
|
|
|
|||
|
|
|
|
|
Legally Blind
Dyspnea With
Minimal Exertion
Other (Specify)
1
2
3
4
5
Complete Bedrest |
6 |
Bedrest BRP |
7 |
Up As Tolerated |
8 |
Transfer Bed/Chair |
9 |
Exercises Prescribed |
|
Partial Weight Bearing |
A |
Independent At Home |
B |
Crutches |
C |
Cane |
D |
Wheelchair
Walker
No Restrictions
Other (Specify)
19. Mental Status |
1 |
Oriented |
3 |
Forgetful |
5 |
Disoriented |
7 |
Agitated |
|
|
|
2 |
Comatose |
4 |
Depressed |
6 |
Lethargic |
8 |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
20. Prognosis |
1 |
Poor |
2 |
Guarded |
3 |
Fair |
4 |
Good |
5 |
Excellent |
21. Orders for Discipline and Treatments (Specify Amount/Frequency/Duration)
22. Goals/Rehabilitation Potential/Discharge Plans
23. Nurse’s Signature and Date of Verbal SOC Where Applicable:
25. Date of HHA Received Signed POT
24. |
Physician’s Name and Address |
26. |
I certify/recertify that this patient is confined to his/her home and needs |
|
|
|
|
intermittent skilled nursing care, physical therapy and/or speech therapy or |
|
|
|
|
continues to need occupational therapy. The patient is under my care, and I have |
|
|
|
|
authorized services on this plan of care and will periodically review the plan. |
|
|
|
|
|
|
27. |
Attending Physician’s Signature and Date Signed |
28. |
Anyone who misrepresents, falsifies, or conceals essential information |
|
|
|
|
required for payment of Federal funds may be subject to fine, imprisonment, |
|
|
|
|
or civil penalty under applicable Federal laws. |
|
|
|
|
|
|
Form
Privacy Act Statement
Sections 1812, 1814, 1815, 1816, 1861 and 1862 of the Social Security Act authorize collection of this information. The primary use of this information is to process and pay Medicare benefits to or on behalf of eligible individuals. Disclosure of this information may be made to: Peer Review Organizations and Quality Review Organizations in connection with their review of claims, or in connection with studies or other review activities, conducted pursuant to Part B of Title XI of the Social Security Act; State Licensing Boards for review of unethical practices or nonprofessional conduct; A congressional office from the record of an individual in response to an inquiry from the congressional office at the request of that individual.
Where the individual’s identification number is his/her Social Security Number (SSN), collection of this information is authorized by Executive Order 9397. Furnishing the information on this form, including the SSN, is voluntary, but failure to do so may result in disapproval of the request for payment of Medicare benefits.
Paper Work Burden Statement
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
| Fact Name | Details |
|---|---|
| Form Purpose | The CMS 485 form is used for home health certification and to create a plan of care for patients requiring home health services. |
| Governing Law | This form is governed by Sections 1812, 1814, 1815, 1816, 1861, and 1862 of the Social Security Act. |
| Patient Information | It collects essential patient information such as name, address, date of birth, and medical record number. |
| Certification Period | The form specifies the start and end dates for the certification period during which home health services are needed. |
| Medications | Details about the patient's medications, including dosage, frequency, and route, are documented on the form. |
| Signature Requirement | Both the attending physician and the nurse must sign the form to validate the plan of care and ensure compliance. |
| Privacy Act Statement | The form includes a Privacy Act Statement that outlines how the information collected will be used and the importance of providing accurate data. |
Completing the CMS 485 form is an important step in ensuring that patients receive the necessary home health care services. This form requires specific information about the patient, their medical condition, and the care they will receive. Once the form is filled out accurately, it will be submitted to the appropriate health care provider or agency for processing.
What is the CMS 485 form used for?
The CMS 485 form, also known as the Home Health Certification and Plan of Care, is utilized to certify a patient's need for home health services. It outlines the patient's medical condition, treatment plan, and the skilled services required, such as nursing care or therapy. This form is essential for Medicare reimbursement and ensures that care is delivered according to the patient's specific needs.
Who needs to sign the CMS 485 form?
The form must be signed by the attending physician who certifies that the patient is homebound and requires intermittent skilled care. The physician’s signature confirms that they have authorized the services outlined in the plan of care and will review the patient's progress periodically.
What information is required on the CMS 485 form?
The CMS 485 form requires several key pieces of information, including the patient's identification details, diagnosis codes, medications, functional limitations, and a detailed plan for care. It also includes sections for safety measures, nutritional requirements, and any allergies the patient may have. This comprehensive information helps ensure appropriate care is provided.
How often should the CMS 485 form be updated?
The CMS 485 form should be updated whenever there is a significant change in the patient's condition or care needs. Additionally, it is typically reviewed and re-signed by the physician every 60 days or as required by Medicare guidelines. Regular updates help maintain accurate and effective care plans.
What happens if the CMS 485 form is not completed correctly?
If the CMS 485 form is not completed accurately, it may lead to delays in service authorization and payment. Incomplete or incorrect information can result in denials of Medicare claims, requiring resubmission of the form. Ensuring all sections are filled out correctly is crucial for timely processing.
Is the information on the CMS 485 form confidential?
Yes, the information provided on the CMS 485 form is protected under privacy laws. The form includes a Privacy Act Statement, which outlines how the information will be used and who may have access to it. This ensures that patient information is handled with confidentiality and care.
How long does it take to complete the CMS 485 form?
Completing the CMS 485 form typically takes about 15 minutes. This estimate includes the time needed to gather necessary information, review instructions, and complete the form. It is important to allocate sufficient time to ensure accuracy and completeness.
Incomplete Patient Information: Failing to provide all necessary patient details, such as the patient's name, address, and date of birth, can lead to processing delays. Ensure that every section is filled out completely.
Incorrect Dates: Entering the wrong start of care date or certification period can cause confusion and may delay services. Double-check these dates for accuracy.
Missing Diagnosis Codes: Not including the appropriate ICD codes for principal and other diagnoses can result in claim denials. It’s crucial to accurately document all relevant medical conditions.
Failure to Document Medications: Omitting details about the patient's medications, including dosage and frequency, can lead to misunderstandings about treatment plans. Be thorough in this section.
Neglecting Functional Limitations: Failing to identify the patient's functional limitations and activities permitted may hinder proper care planning. Clearly outline any restrictions.
Inaccurate Prognosis: Providing an unrealistic prognosis can mislead care providers and affect the patient's treatment plan. Be honest and accurate in your assessment.
Signature Issues: Not obtaining the necessary signatures from the attending physician or nurse can invalidate the form. Ensure that all required signatures are collected before submission.
The CMS 485 form, also known as the Home Health Certification and Plan of Care, is a crucial document used in the home health care process. It outlines the patient's medical needs and the care plan designed to address those needs. Alongside this form, several other documents are often required to ensure comprehensive care and compliance with Medicare regulations. Below is a list of commonly associated forms that play a vital role in the home health care process.
Understanding these forms and documents is essential for anyone involved in home health care. Each one plays a specific role in ensuring that patients receive the best possible care while also meeting regulatory requirements. Properly managing these documents can lead to improved patient outcomes and smoother operational processes within home health agencies.
When filling out the CMS 485 form, it's essential to approach the task with care and attention. Here are five things you should and shouldn't do to ensure the form is completed correctly.
The CMS 485 form is a critical document for home health care providers, yet several misconceptions surround its purpose and requirements. Here are six common misunderstandings:
Understanding these misconceptions can help patients and providers navigate the complexities of home health care more effectively.
Here are some important points to remember when filling out and using the CMS 485 form: