The California PM110 form serves as a crucial tool for healthcare providers in reporting various communicable diseases and conditions that pose a public health risk. Designed by the California Department of Public Health, this form is not just a bureaucratic requirement; it plays a vital role in tracking diseases such as sexually transmitted infections, hepatitis, and tuberculosis. When completing the PM110, healthcare providers must include essential patient information, including demographics, disease specifics, and treatment details. The form also outlines specific reporting requirements, emphasizing the urgency of notifying local health authorities about certain diseases. Failure to report can lead to significant legal consequences, underscoring the importance of compliance. Additionally, the PM110 includes sections dedicated to sexually transmitted diseases and tuberculosis, ensuring that healthcare providers can provide detailed information relevant to these conditions. By understanding the PM110 form and its requirements, healthcare professionals can contribute effectively to public health efforts and help contain outbreaks before they escalate.
State of
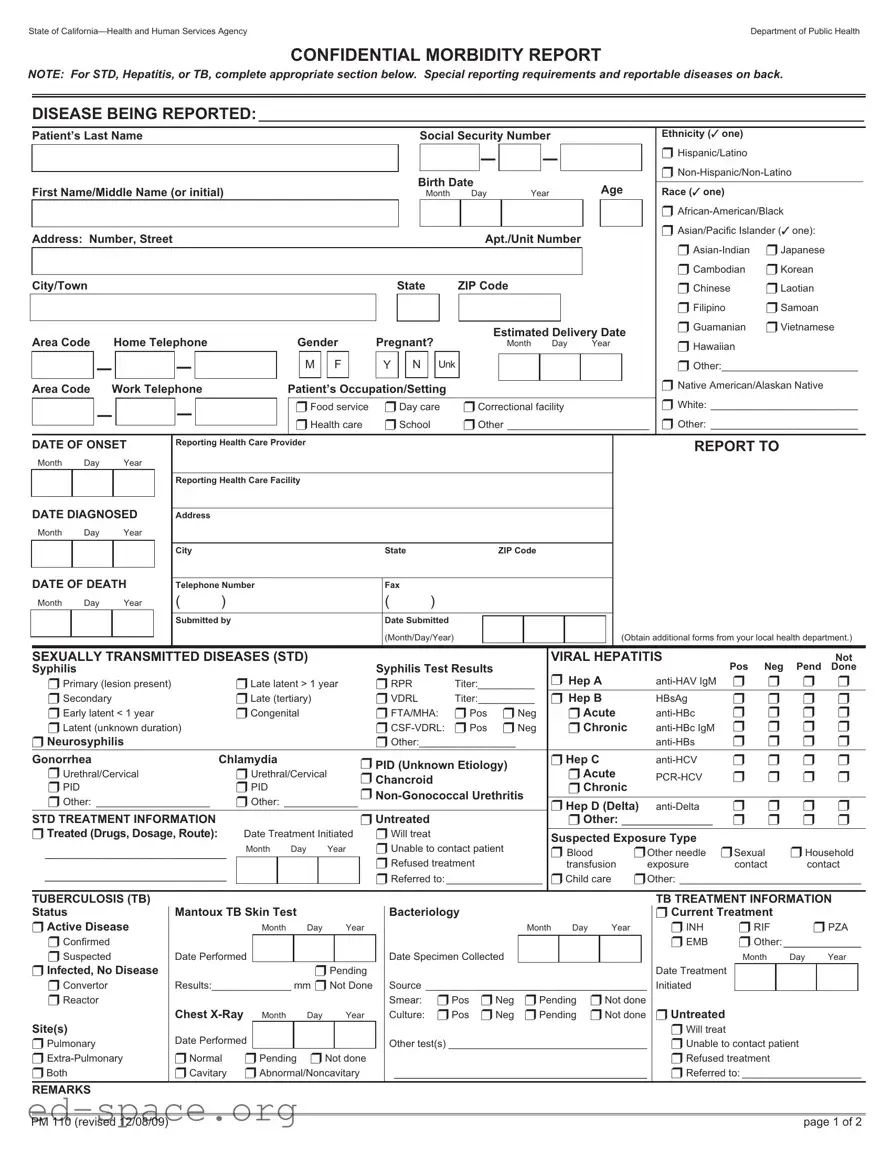
CONFIDENTIAL MORBIDITY REPORT
NOTE: For STD, Hepatitis, or TB, complete appropriate section below. Special reporting requirements and reportable diseases onback.
DISEASE BEING REPORTED:___________________________________________________________________________________
Patient’s Last Name |
Social Security Number |
Ethnicity (✓ one) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
– |
|
|
– |
|
|
|
|
|
|
|
|
|
|
|
❒ Hispanic/Latino |
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Birth Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Age |
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
First Name/Middle Name (or initial) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Race (✓ one) |
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Month |
|
Day |
|
|
|
Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Asian/Pacific Islander (✓ one): |
|
|
|
||||||
Address: Number, Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Apt./Unit Number |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ |
❒ Japanese |
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Cambodian |
❒ Korean |
|
|
|
|||||
City/Town |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
|
|
ZIP Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Chinese |
❒ Laotian |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Filipino |
❒ Samoan |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Guamanian |
❒ Vietnamese |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Estimated Delivery Date |
|
|
|
|
|||||||||||||||||||||||||
Area Code |
Home Telephone |
|
|
|
|
|
Gender |
Pregnant? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
Month |
Day |
Year |
|
|
|
|
❒ Hawaiian |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
– |
|
|
|
– |
|
|
|
|
|
|
|
M |
|
|
F |
|
|
|
Y |
|
N |
|
|
Unk |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Other:________________________ |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Native American/Alaskan Native |
|
|
|
||||||
Area Code |
Work Telephone |
|
|
|
|
Patient’s Occupation/Setting |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ White: __________________________ |
||||||||||||
|
|
|
– |
|
|
|
– |
|
|
|
|
|
|
❒Food service |
|
|
❒Day care |
|
❒Correctional facility |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
❒Health care |
|
|
❒School |
|
❒Other _________________________ |
|
❒ Other: __________________________ |
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF ONSET |
Reporting Health Care Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REPORT TO |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Month |
Day |
Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Reporting Health Care Facility |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE DIAGNOSED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Month |
Day |
Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
|
|
|
|
|
|
|
ZIP Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
DATE OF DEATH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Telephone Number |
|
|
|
|
|
|
|
|
|
|
|
Fax |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Month |
Day |
Year |
( |
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
|
|
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Submitted by |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date Submitted |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Month/Day/Year) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Obtain additional forms from your local health department.) |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SEXUALLY TRANSMITTED DISEASES (STD) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VIRAL HEPATITIS |
|
|
|
|
|
|
Not |
||||||||||||||||||||||||||||||||
Syphilis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Syphilis Test Results |
|
|
|
|
|
|
|
❒ Hep A |
|
|
|
|
|
Pos |
Neg |
Pend |
Done |
|||||||||||||||||||||||||||
❒ Primary (lesion present) |
|
|
|
❒Late latent > 1 year |
❒ RPR |
|
|
|
|
Titer:__________ |
|
|
|
|
|
❒ |
❒ |
❒ |
❒ |
||||||||||||||||||||||||||||||||||||||||||||||
❒ Secondary |
|
|
|
|
|
|
❒Late (tertiary) |
|
|
|
|
❒ VDRL |
|
|
|
|
Titer:__________ |
|
❒ Hep B |
|
|
|
HBsAg |
❒ |
❒ |
❒ |
❒ |
||||||||||||||||||||||||||||||||||||||
❒ Early latent < 1 year |
|
|
|
❒Congenital |
|
|
|
|
❒ FTA/MHA: |
❒ Pos |
|
❒ Neg |
|
|
|
❒ Acute |
|
|
|
❒ |
❒ |
❒ |
❒ |
||||||||||||||||||||||||||||||||||||||||||
❒ Latent (unknown duration) |
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ |
❒ Pos |
|
❒ Neg |
|
|
|
❒ Chronic |
|
|
|
❒ |
❒ |
❒ |
❒ |
|||||||||||||||||||||||||||||||||||||
❒ Neurosyphilis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Other:_________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ |
❒ |
❒ |
❒ |
|||||||||||||||||||||||||||||
Gonorrhea |
|
|
|
|
|
Chlamydia |
|
|
|
|
|
|
|
|
❒ PID (Unknown Etiology) |
|
|
|
|
❒ Hep C |
|
|
|
❒ |
❒ |
❒ |
❒ |
||||||||||||||||||||||||||||||||||||||
❒ Urethral/Cervical |
|
|
|
❒ Urethral/Cervical |
|
|
|
|
|
|
|
|
|
❒ Acute |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
❒ Chancroid |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ |
❒ |
❒ |
❒ |
|||||||||||||||||||||||||||||||||||||||
❒ PID |
|
|
|
|
|
|
|
|
❒ PID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Chronic |
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
❒ Other: ____________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
❒ Other: _____________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Hep D (Delta) |
❒ |
❒ |
❒ |
❒ |
||||||||||||||||||||||||||||||||||||||
STD TREATMENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
❒ Untreated |
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Other: ______________ |
❒ |
❒ |
❒ |
❒ |
||||||||||||||||||||||||||||||||||
❒ Treated(Drugs,Dosage,Route): |
|
Date Treatment Initiated |
❒ Will treat |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Suspected Exposure Type |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Unable to contact patient |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
____________________________ |
Month |
Day |
Year |
|
|
|
|
❒ Blood |
❒Other needle |
❒Sexual |
❒ Household |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Refused treatment |
|
|
|
|
|
|
|
|
|
|
|
transfusion |
|
exposure |
contact |
contact |
|||||||||||||||||||||||||||
____________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
❒ Referred to:_________________ |
|
❒Child care |
❒Other: ________________________________ |
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TUBERCULOSIS (TB) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TB TREATMENT INFORMATION |
||||||||||||||||
Status |
|
|
|
|
|
Mantoux TB Skin Test |
|
|
|
|
|
|
Bacteriology |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Current Treatment |
|
|
|
|
|
|||||||||||||||||||||||||
❒ Active Disease |
|
|
|
|
|
Month |
|
|
Day |
|
Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Month Day |
|
|
Year |
|
|
|
|
❒ INH |
|
❒ RIF |
❒ PZA |
|||||||||||||||||||||||||
❒ Confirmed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ EMB |
|
❒ Other:____________ |
||||||||||
❒ Suspected |
|
|
|
Date Performed |
|
|
|
|
|
|
|
|
|
|
|
|
|
Date Specimen Collected |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Month |
Day |
Year |
||||||||||||||||||||||||
❒ Infected, No Disease |
|
|
|
|
|
|
|
|
|
❒ Pending |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date Treatment |
|
|
|
|
|
|
|
|
|||||||||||||
❒ Convertor |
|
|
|
Results:______________ mm ❒ Not Done |
|
|
Source _______________________________________ |
|
Initiated |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
❒ Reactor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Smear: |
|
|
❒Pos |
❒Neg |
❒Pending |
❒Not done |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
Chest |
|
|
Day |
|
Year |
|
|
Culture: |
|
|
❒Pos |
❒Neg |
❒Pending |
❒Not done |
|
❒ Untreated |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
Site(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Will treat |
|
|
|
|
|
|
|
|||
❒ Pulmonary |
|
|
|
Date Performed |
|
|
|
|
|
|
|
|
|
|
|
|
|
Other test(s) ___________________________________ |
|
|
❒ Unable to contact patient |
|
|
|
|||||||||||||||||||||||||||||||||||||||||
❒ |
|
❒Normal |
❒Pending ❒Not done |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❒ Refused treatment |
|
|
|
|
|
||||||||||||||||||||||
❒Both |
|
|
|
|
|
❒Cavitary |
❒Abnormal/Noncavitary |
|
_______________________________________ |
|
|
❒ Referred to:_____________________ |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REMARKS
PM 110 (revised 12/08/09) |
page 1 of 2 |
| Fact Name | Details |
|---|---|
| Purpose | The California PM110 form is used for reporting certain communicable diseases, including sexually transmitted diseases, viral hepatitis, and tuberculosis, to local health authorities. |
| Governing Laws | This form is governed by Title 17 of the California Code of Regulations, specifically sections 2500, 2593, and 2641.5-2643.20, which outline reporting requirements for health care providers. |
| Confidentiality | Information submitted on the PM110 form is confidential and is intended for use by health authorities to monitor and control the spread of diseases. |
| Reporting Timeline | Health care providers must report cases of specified diseases within certain timeframes, such as within one working day for urgent cases, as outlined in section 2500 of the regulations. |
| Consequences of Non-Compliance | Failure to report as mandated can lead to misdemeanor charges and civil penalties, emphasizing the importance of timely and accurate reporting. |
After gathering all necessary information, you can proceed to fill out the California PM110 form. Ensure that you have accurate details about the patient and the disease being reported. Follow the steps below to complete the form correctly.
What is the California PM110 form?
The California PM110 form is a confidential morbidity report used by healthcare providers to report certain communicable diseases to the local health department. This form is essential for tracking and managing public health concerns, including sexually transmitted diseases (STDs), viral hepatitis, and tuberculosis (TB). It ensures that health authorities can monitor disease outbreaks and implement necessary interventions.
Who is required to complete the PM110 form?
Any healthcare provider who is aware of or attending to a case of a reportable disease must complete the PM110 form. This includes physicians, nurse practitioners, and other medical professionals. If no healthcare provider is present, any individual who knows about a suspected case can report it. This broad requirement helps ensure that all cases are documented and reported promptly.
What types of diseases must be reported using the PM110 form?
The PM110 form is specifically designed for reporting various communicable diseases, including but not limited to STDs like syphilis and chlamydia, viral hepatitis types A, B, and C, and tuberculosis. A complete list of reportable diseases is provided on the back of the form and includes many other conditions that pose a risk to public health.
How quickly must a report be submitted?
Reporting timelines vary depending on the disease. Some diseases must be reported immediately by phone, while others can be reported within one working day or seven calendar days after identification. The urgency of the report depends on the disease's potential impact on public health and safety.
What information is required on the PM110 form?
The form collects essential information about the patient, including their name, date of birth, ethnicity, and address. Additionally, it requires details about the disease being reported, the healthcare provider’s information, and any relevant test results. This comprehensive data helps health officials understand the scope of the issue and respond accordingly.
What happens if a healthcare provider fails to report a case?
Failure to report a case using the PM110 form is considered a misdemeanor and can result in penalties. Healthcare providers may face fines or other legal consequences for not complying with reporting requirements. This emphasizes the importance of timely and accurate reporting to protect public health.
Where can I obtain more PM110 forms?
Healthcare providers can obtain additional copies of the PM110 form from their local health department. It is also available online through the California Department of Public Health’s website. Ensuring that the correct forms are readily available helps facilitate the reporting process and supports public health initiatives.
Incomplete Patient Information: Failing to provide all necessary details such as the patient's last name, date of birth, and social security number can lead to processing delays. Each piece of information is crucial for accurate identification.
Incorrect Disease Identification: Misreporting the disease being reported or selecting the wrong category can result in confusion and mismanagement of public health responses. It's essential to ensure the correct disease is marked clearly.
Missing or Incorrect Dates: Omitting important dates, such as the date of onset or date diagnosed, can hinder the investigation process. All dates must be filled in accurately to ensure proper tracking and follow-up.
Failure to Indicate Treatment Status: Not specifying whether the patient has been treated or is untreated can lead to miscommunication regarding the urgency of the case. Treatment status should be clearly indicated to inform health authorities.
Inaccurate Contact Information: Providing incorrect or outdated contact information for the reporting health care provider can create obstacles in communication. Always double-check that the phone numbers and addresses are accurate.
Neglecting to Report Urgent Cases: Some diseases require immediate reporting. Failing to recognize and report these cases promptly can jeopardize public health. Be aware of the urgency requirements for specific diseases.
Overlooking Special Reporting Requirements: Certain diseases have specific reporting guidelines. Ignoring these can lead to incomplete reports. Familiarize yourself with any special requirements associated with the disease being reported.
Not Keeping a Copy of the Submitted Form: Failing to retain a copy of the submitted PM110 form can cause issues if follow-up is needed. Always keep a record for your files to ensure you have documentation of what was reported.
The California PM110 form is a crucial document for reporting certain communicable diseases. When dealing with public health, various other forms and documents often accompany the PM110 to ensure comprehensive reporting and management of health concerns. Here’s a list of some of these important documents:
Using these forms in conjunction with the PM110 helps health authorities maintain accurate records and respond effectively to public health issues. Each document serves a specific purpose, contributing to a broader understanding of health trends and risks in California.
The California PM110 form is designed for the reporting of communicable diseases and conditions. It shares similarities with several other documents used in public health reporting. Below are four documents that are comparable to the PM110 form:
When filling out the California PM110 form, it's important to follow specific guidelines to ensure accuracy and compliance. Here’s a list of things to do and avoid:
This form is actually used for reporting various communicable diseases, including tuberculosis and hepatitis, not just STDs.
Any health care provider, including nurses and physician assistants, can complete this form if they are aware of a reportable disease.
In fact, the PM110 form is designed to maintain patient confidentiality while reporting necessary health information.
Reporting is mandatory for health care providers who know of a case or suspected case of a reportable disease.
Providers should report suspected cases as well, not just confirmed diagnoses.
There are specific time frames for reporting different diseases, which providers must follow to ensure timely public health responses.
Only health care providers or individuals with knowledge of a case can submit the form to the local health officer.
When filling out and using the California PM110 form, keep these key takeaways in mind: