The California CDPH 4461 form plays a crucial role in determining eligibility for the Family PACT Program, which provides essential family planning services. Designed by the California Department of Public Health, this form collects vital information about the applicant's family size, income, and health care insurance status. It is important to answer all questions accurately, as the information will be used to assess eligibility for the program. The form also emphasizes confidentiality, allowing applicants to indicate if they need their family planning services kept private from partners or family members. Additionally, it includes sections for personal identification, income sources, and family member details, ensuring a comprehensive understanding of the applicant's situation. Providers are required to keep a copy of the completed form in the client’s medical record, maintaining the integrity of the application process. Understanding the significance of this form can empower individuals to access the necessary services they need.
State of |
California Department of Public Health |
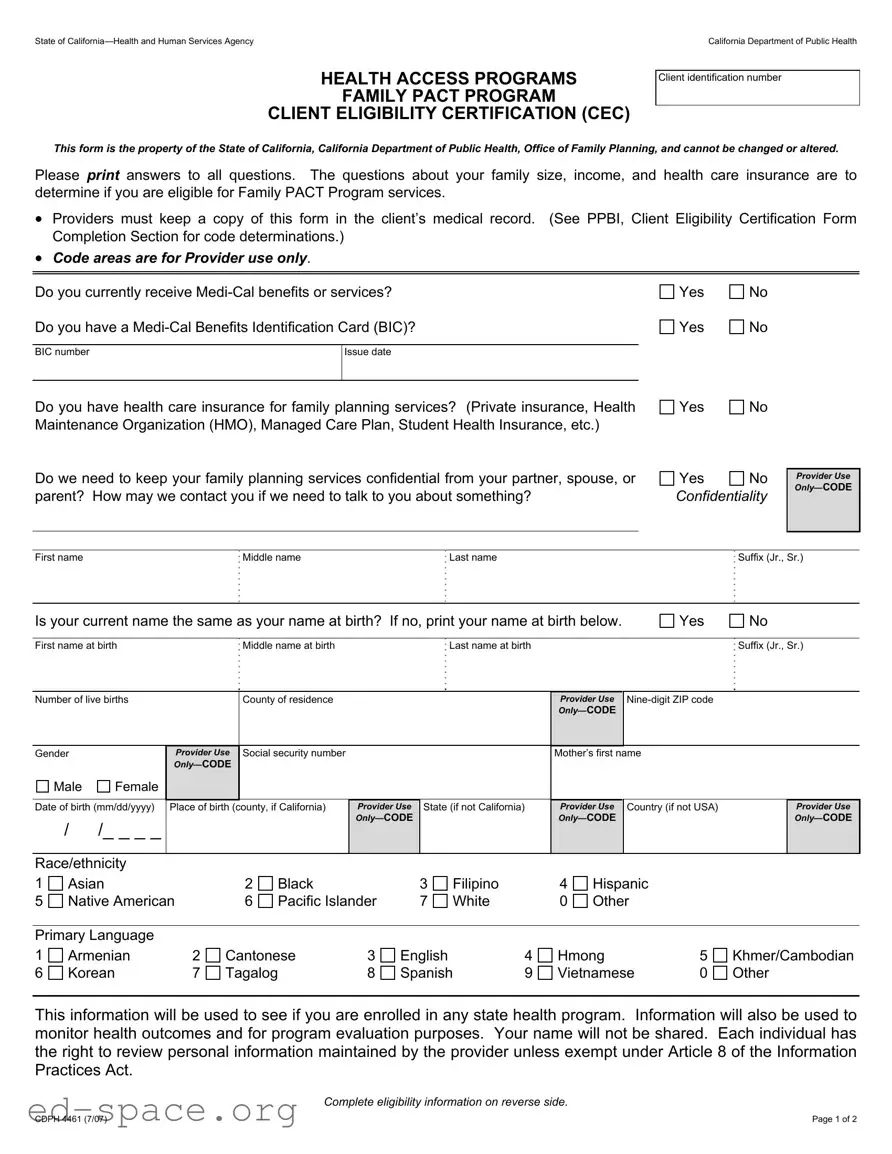
HEALTH ACCESS PROGRAMS
FAMILY PACT PROGRAM
CLIENT ELIGIBILITY CERTIFICATION (CEC)
Client identification number
This form is the property of the State of California, California Department of Public Health, Office of Family Planning, and cannot be changed or altered.
Please print answers to all questions. The questions about your family size, income, and health care insurance are to determine if you are eligible for Family PACT Program services.
•Providers must keep a copy of this form in the client’s medical record. (See PPBI, Client Eligibility Certification Form Completion Section for code determinations.)
•Code areas are for Provider use only.
Do you currently receive
Do you have a
BIC number |
Issue date |
|
|
Do you have health care insurance for family planning services? (Private insurance, Health Maintenance Organization (HMO), Managed Care Plan, Student Health Insurance, etc.)
Do we need to keep your family planning services confidential from your partner, spouse, or parent? How may we contact you if we need to talk to you about something?
Yes |
No |
Yes |
No |
Yes |
No |
Yes |
No |
Confidentiality
Provider Use
First name |
Middle name |
Last name |
Suffix (Jr., Sr.) |
Is your current name the same as your name at birth? If no, print your name at birth below.
Yes
No
First name at birth |
Middle name at birth |
Last name at birth |
Suffix (Jr., Sr.) |
Number of live births
Gender
Male Female
Provider Use
County of residence
Social security number
Provider Use
Mother’s first name
Date of birth (mm/dd/yyyy)
//_ _ _ _
Place of birth (county, if California)
Provider Use
State (if not California)
Provider Use
Country (if not USA)
Provider Use
Race/ethnicity |
|
|
|
|
|
|
|
|
|
|
|
|
1 |
Asian |
|
2 |
Black |
|
3 |
Filipino |
|
4 |
Hispanic |
|
|
5 |
Native American |
|
6 |
Pacific Islander |
7 |
White |
|
0 |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary Language |
|
|
|
|
|
|
|
|
|
|
|
|
1 |
Armenian |
2 |
Cantonese |
3 |
English |
|
4 |
Hmong |
5 |
Khmer/Cambodian |
||
6 |
Korean |
7 |
Tagalog |
8 |
Spanish |
9 |
Vietnamese |
0 |
Other |
|||
This information will be used to see if you are enrolled in any state health program. Information will also be used to monitor health outcomes and for program evaluation purposes. Your name will not be shared. Each individual has the right to review personal information maintained by the provider unless exempt under Article 8 of the Information Practices Act.
Complete eligibility information on reverse side.
CDPH 4461 (7/07) |
Page 1 of 2 |
Eligibility Determination: Please list all family members (self, spouse, and children) living in your household and supported by the family income. List the source of any earned or unearned income and the amount of income, including income from employment,
Name
Relationship to You
Age
Source of Income
Gross Monthly Income
(Before taxes or deductions.)
(Self)
Family size:
Total family income $
I declare under penalty of perjury that the information I have given on this form is true, correct, and complete. I understand that the giving of false information may make me ineligible for this program.
Signature (or mark) of applicant
Date
Signature of witness to mark or interpreter
Date
Provider certification:
FOR PROVIDER USE ONLY
Eligible for Family PACT Program
Ineligible for Family PACT Program (Give applicant Fair Hearing Rights.)
Limited scope
Unmet
Based upon the information provided by the applicant and according to state and federal requirements, I certify that the applicant identified on this Client Eligibility Certification is eligible to receive family planning services under the Family PACT Program. If ineligible, the client has received a copy of this form which includes the Fair Hearing Rights.
Print name |
Signature |
Date |
|
||
|
|
|
|
|
|
|
|
Date |
Reason code (see Provider |
|
|
Annual Certification: If client is decertified (no longer eligible) |
|
Manual) |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
Fair Hearing Rights
Any applicant for, or recipient of, services under the Family PACT Program has a right to a hearing conducted by the California Department of Public Health regarding eligibility or receipt of services. An applicant or recipient does not have a right to contest changes made to the eligibility standards or benefits of the Family PACT Program.
First level review: If you wish to appeal either your denial of eligibility or receipt of services, please send your name, telephone number, address, and reason why you are requesting a review to the First Level Review address below. A request for a first level review must be postmarked within 20 working days of the denial of eligibility or services. The Office of Family Planning may request additional information by telephone or in writing from the provider or the applicant before issuing a decision.
Formal hearing: You may appeal the decision of the first level review within five working days of your receipt of the decision of the first level review by sending your name, telephone number, address, and reason for the appeal to the Formal Hearing address below. At the hearing, you may be represented by a friend, relative, lawyer, or other person of your choice. A representative of the provider will be present to explain the reasons for denying eligibility. If you want an interpreter provided at the hearing, please specify the language in your letter requesting a hearing.
First Level Review |
Formal Hearing |
California Department of Public Health |
California Department of Public Health |
Office of Family Planning |
Office of Regulations and Hearings |
MS 8400 |
MS 0507 |
P.O. Box 997420 |
P.O. Box 997377 |
Sacramento, CA |
Sacramento, CA |
CDPH 4461 (7/07) |
Page 2 of 2 |
| Fact Name | Description |
|---|---|
| Form Purpose | The California CDPH 4461 form is used to certify client eligibility for the Family PACT Program, which provides family planning services. |
| Confidentiality | Clients can request confidentiality regarding their family planning services from partners, spouses, or parents. |
| Provider Responsibilities | Providers must keep a copy of the completed form in the client's medical record to ensure proper documentation and compliance. |
| Eligibility Criteria | The form collects information about family size, income, and health care insurance to determine eligibility for services. |
| Legal Authority | This form is governed by California Health and Safety Code, Section 24000, which outlines the Family PACT Program requirements. |
| Appeal Process | Applicants have the right to appeal eligibility decisions through a first level review and a formal hearing, as outlined in the form. |
Completing the California CDPH 4461 form requires careful attention to detail. This form is essential for determining eligibility for the Family PACT Program. Follow these steps to ensure that all necessary information is provided accurately.
Once you have completed the form, it will be submitted for processing. The information you provide will be used to assess your eligibility for the Family PACT Program. It is important to ensure that all details are accurate, as any discrepancies may affect your application.
What is the California CDPH 4461 form?
The California CDPH 4461 form is the Client Eligibility Certification (CEC) used for the Family PACT Program. This program provides family planning services to eligible individuals in California. The form collects essential information about the applicant's family size, income, and health care insurance to determine eligibility for these services.
Who needs to fill out the CDPH 4461 form?
Individuals seeking family planning services under the Family PACT Program must complete the CDPH 4461 form. This includes those who may not currently have health insurance or are looking for additional family planning support. It is crucial for applicants to provide accurate information to ensure proper eligibility assessment.
How is the information on the CDPH 4461 form used?
The information collected on the CDPH 4461 form is used to determine if an individual qualifies for the Family PACT Program. It helps assess family size, income levels, and existing health care coverage. Additionally, the data may be used for monitoring health outcomes and program evaluation, although personal details remain confidential.
What happens if I provide false information on the form?
Providing false information on the CDPH 4461 form can lead to ineligibility for the Family PACT Program. Applicants must declare that the information given is true and complete, as any discrepancies may result in denial of services. It is essential to be honest to avoid potential penalties.
Can I keep my family planning services confidential?
Yes, the CDPH 4461 form includes a question regarding confidentiality. If you need your family planning services to remain confidential from a partner, spouse, or parent, you can indicate this on the form. Your privacy is taken seriously, and measures will be taken to protect your information.
What should I do if I am denied eligibility for the Family PACT Program?
If your eligibility for the Family PACT Program is denied, you have the right to appeal the decision. You can request a first-level review by sending your name, contact information, and reason for the appeal to the Office of Family Planning within 20 working days of the denial. If you disagree with the outcome of the first-level review, you may appeal further through a formal hearing.
Where can I find more information about the Family PACT Program?
For additional details about the Family PACT Program and the CDPH 4461 form, you can visit the California Department of Public Health's website. There, you will find resources, eligibility criteria, and contact information for assistance. It is advisable to stay informed about the program's updates and requirements.
Neglecting to Provide Complete Information: One common mistake is leaving sections blank or providing incomplete answers. Each question is important for determining eligibility, so ensure that all fields are filled out accurately.
Incorrectly Reporting Income: Applicants often miscalculate their total family income. It's crucial to include all sources of income, such as employment, pensions, and benefits. Double-check your figures to avoid errors.
Forgetting to Sign the Form: A signature is required to certify that the information provided is true and complete. Without a signature, the form cannot be processed, leading to delays or denial of services.
Not Keeping a Copy: Failing to retain a copy of the completed form can lead to confusion later. It's advisable to keep a personal record for future reference and to track your eligibility status.
Overlooking Confidentiality Options: Some applicants may not indicate if they require confidentiality regarding their family planning services. If privacy is a concern, make sure to clearly state this on the form.
The California CDPH 4461 form is essential for determining eligibility for the Family PACT Program. Alongside this form, several other documents may be required or helpful in the process. Below is a list of related forms and documents that are often used in conjunction with the CDPH 4461.
Having these documents ready can streamline the process of applying for and receiving services under the Family PACT Program. Each document serves a specific purpose and helps ensure that clients receive the support they need.
The California CDPH 4461 form serves a specific purpose in determining eligibility for the Family PACT Program. Several other documents share similarities with this form, primarily in their function of gathering personal and financial information for eligibility assessments. Below is a list of six documents that are comparable to the CDPH 4461 form:
When filling out the California CDPH 4461 form, it’s important to be thorough and accurate. Here’s a helpful list of things you should and shouldn’t do to ensure your application is processed smoothly.
Completing the form accurately is essential for determining your eligibility for the Family PACT Program. Taking the time to follow these guidelines will help streamline the process and reduce any potential delays.
Misconception 1: The CDPH 4461 form is only for low-income individuals.
This form is designed for anyone seeking eligibility for the Family PACT Program, not just those with low income. It considers various factors, including family size and health care insurance, to determine eligibility.
Misconception 2: Filling out the form guarantees eligibility for services.
Submitting the CDPH 4461 form does not automatically mean you will qualify for the Family PACT Program. Eligibility is determined based on the information provided and compliance with state and federal requirements.
Misconception 3: The information on the form will be shared with others.
Your personal information is kept confidential. The form states that your name will not be shared, ensuring your privacy throughout the process.
Misconception 4: You cannot appeal a denial of services.
You do have the right to appeal if your eligibility is denied. The process includes a first-level review and the option for a formal hearing if needed.
Misconception 5: The form is only for women.
The CDPH 4461 form is applicable to all individuals, regardless of gender. It is meant for anyone seeking family planning services under the Family PACT Program.
Understanding the California CDPH 4461 form is essential for those seeking services under the Family PACT Program. Here are key takeaways to consider when filling out and using this important document: