The California Audit form is a vital tool for individuals seeking to address concerns related to workers' compensation claims. This form allows injured workers to formally lodge complaints against claims administrators regarding various issues, such as delayed payments, denial of medical treatment, or inadequate investigations. One of the key features of the form is the option for complainants to request confidentiality, ensuring that their identity remains protected throughout the process. The information collected is utilized by the Department of Industrial Relations to monitor compliance and assist in law enforcement efforts. It's important to provide specific details about the nature of the complaint, including any relevant dates and documentation, to facilitate a thorough review. The form also requires basic identifying information about the injured worker, the claims administrator, and the employer involved. By filling out this form accurately, individuals can help improve the workers' compensation system while ensuring their grievances are heard and addressed.
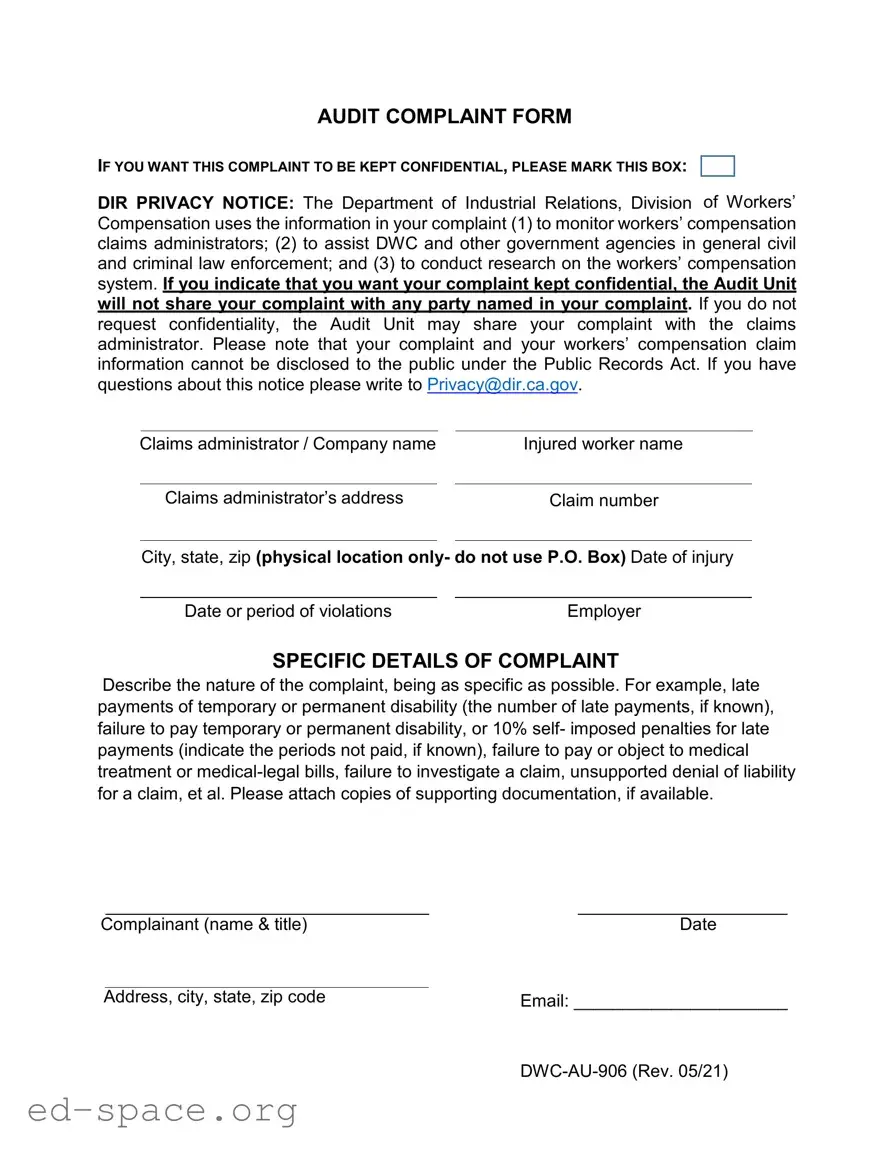
AUDIT COMPLAINT FORM
IF YOU WANT THIS COMPLAINT TO BE KEPT CONFIDENTIAL, PLEASE MARK THIS BOX:
DIR PRIVACY NOTICE: The Department of Industrial Relations, Division of Workers’ Compensation uses the information in your complaint (1) to monitor workers’ compensation claims administrators; (2) to assist DWC and other government agencies in general civil and criminal law enforcement; and (3) to conduct research on the workers’ compensation system. If you indicate that you want your complaint kept confidential, the Audit Unit will not share your complaint with any party named in your complaint. If you do not request confidentiality, the Audit Unit may share your complaint with the claims administrator. Please note that your complaint and your workers’ compensation claim information cannot be disclosed to the public under the Public Records Act. If you have questions about this notice please write to [email protected].
Claims administrator / Company name
Claims administrator’s address
Injured worker name
Claim number
City, state, zip (physical location only- do not use P.O. Box) Date of injury
Date or period of violations |
Employer |
SPECIFIC DETAILS OF COMPLAINT
Describe the nature of the complaint, being as specific as possible. For example, late payments of temporary or permanent disability (the number of late payments, if known), failure to pay temporary or permanent disability, or 10% self- imposed penalties for late payments (indicate the periods not paid, if known), failure to pay or object to medical treatment or
Complainant (name & title) |
Date |
Address, city, state, zip code |
Email: ______________________ |
|
| Fact Name | Description |
|---|---|
| Purpose of the Form | The California Audit Complaint Form is designed for individuals to report issues related to workers' compensation claims. |
| Confidentiality Option | Complainants can request confidentiality for their complaints, ensuring that their identity remains protected. |
| Governing Law | This form is governed by California Labor Code Section 129.5, which outlines the rights of injured workers. |
| Information Usage | The Department of Industrial Relations uses the information to monitor claims administrators and assist in law enforcement. |
| Public Disclosure | Complaints and workers' compensation claim information are not subject to public disclosure under the Public Records Act. |
| Supporting Documentation | Complainants are encouraged to attach copies of any supporting documentation to strengthen their case. |
| Specific Complaint Details | Detailing the nature of the complaint is essential; specifics can include late payments or denial of claims. |
| Contact Information | Complainants must provide their name, title, address, and email to facilitate communication. |
| Revocation Date | The form was last revised in May 2021, indicating it may be subject to updates in response to changing laws or practices. |
Filling out the California Audit form is an important step in addressing your complaint regarding workers' compensation issues. After submitting the form, the relevant authorities will review your complaint and take appropriate action based on the information provided.
What is the purpose of the California Audit Complaint Form?
The California Audit Complaint Form is designed to allow individuals to report issues related to workers' compensation claims. This form serves multiple purposes, including monitoring the performance of claims administrators, assisting in law enforcement efforts, and facilitating research on the workers' compensation system. By filing a complaint, you contribute to the oversight of how claims are managed and ensure accountability within the system.
How can I keep my complaint confidential?
If you wish to keep your complaint confidential, you must mark the designated box on the form. By doing this, the Audit Unit will not disclose your complaint to any parties mentioned in it, including the claims administrator. However, if you choose not to request confidentiality, your complaint may be shared with the claims administrator involved in your case. It is important to note that, regardless of your choice, your complaint and related information are not public records and cannot be disclosed under the Public Records Act.
What information should I include in the complaint?
What happens after I submit the complaint?
Once the complaint is submitted, the Audit Unit will review the information provided. They may use the details to investigate the claims administrator's practices and determine if any violations have occurred. Depending on the findings, the Audit Unit may take appropriate action, which could include further inquiries or enforcement measures. You may not receive direct updates about the outcome of your complaint, but rest assured that your submission contributes to the overall monitoring of the workers' compensation system.
Who should I contact if I have questions about the privacy notice?
If you have questions or concerns regarding the privacy notice associated with the California Audit Complaint Form, you can reach out directly to the Department of Industrial Relations at the email address provided: [email protected]. They can provide clarification on how your information is handled and the implications of requesting confidentiality for your complaint.
Not marking the confidentiality box: If you want your complaint to be confidential, it is crucial to mark the designated box. Failing to do so means your complaint could be shared with the claims administrator.
Providing incomplete information: Ensure that all required fields, such as the claims administrator's name, address, and the injured worker's details, are filled out completely. Missing information can delay the processing of your complaint.
Using a P.O. Box for the address: The form specifically requests a physical location. Using a P.O. Box instead of a physical address can lead to complications or rejections of your submission.
Being vague in the complaint description: When describing the nature of your complaint, detail is key. Vague descriptions can result in misunderstandings or insufficient action being taken.
Not attaching supporting documentation: If you have any evidence to support your claims, such as payment records or correspondence, be sure to attach them. This documentation can significantly strengthen your case.
Failing to include contact information: Providing your email address and other contact details is essential. Without this information, the Audit Unit may have difficulty reaching you for follow-up questions.
Ignoring the date of injury: Make sure to include the correct date of injury. This information is vital for the Audit Unit to assess the timeline of your complaint accurately.
Not specifying the periods of violations: If your complaint involves late payments or other violations, indicate the specific periods during which these occurred. This clarity helps in evaluating your case.
Neglecting to proofread the form: Before submitting, take a moment to review the form for any errors or omissions. Small mistakes can lead to significant delays in processing your complaint.
When dealing with a California Audit form, several other documents may be necessary to support your case or provide additional information. Understanding these documents can help streamline your process and ensure that all relevant information is submitted correctly. Below is a list of commonly used forms and documents that accompany the California Audit form.
Gathering these documents alongside the California Audit form can significantly enhance your case. Make sure to keep everything organized and accessible, as this will facilitate a smoother review process and increase the likelihood of a favorable outcome.
The California Audit form shares similarities with several other documents used in various contexts. Each of these documents serves a specific purpose related to reporting or filing complaints. Below are five documents that are similar to the California Audit form:
When filling out the California Audit form, certain practices can enhance the effectiveness of your complaint. Conversely, some actions may hinder your submission. Here’s a list of what to do and what to avoid.
Understanding the California Audit form can be challenging, and several misconceptions often arise. Here are five common misunderstandings about this important document:
Filling out the California Audit form requires careful attention to detail and an understanding of the process involved. Here are some key takeaways to consider: