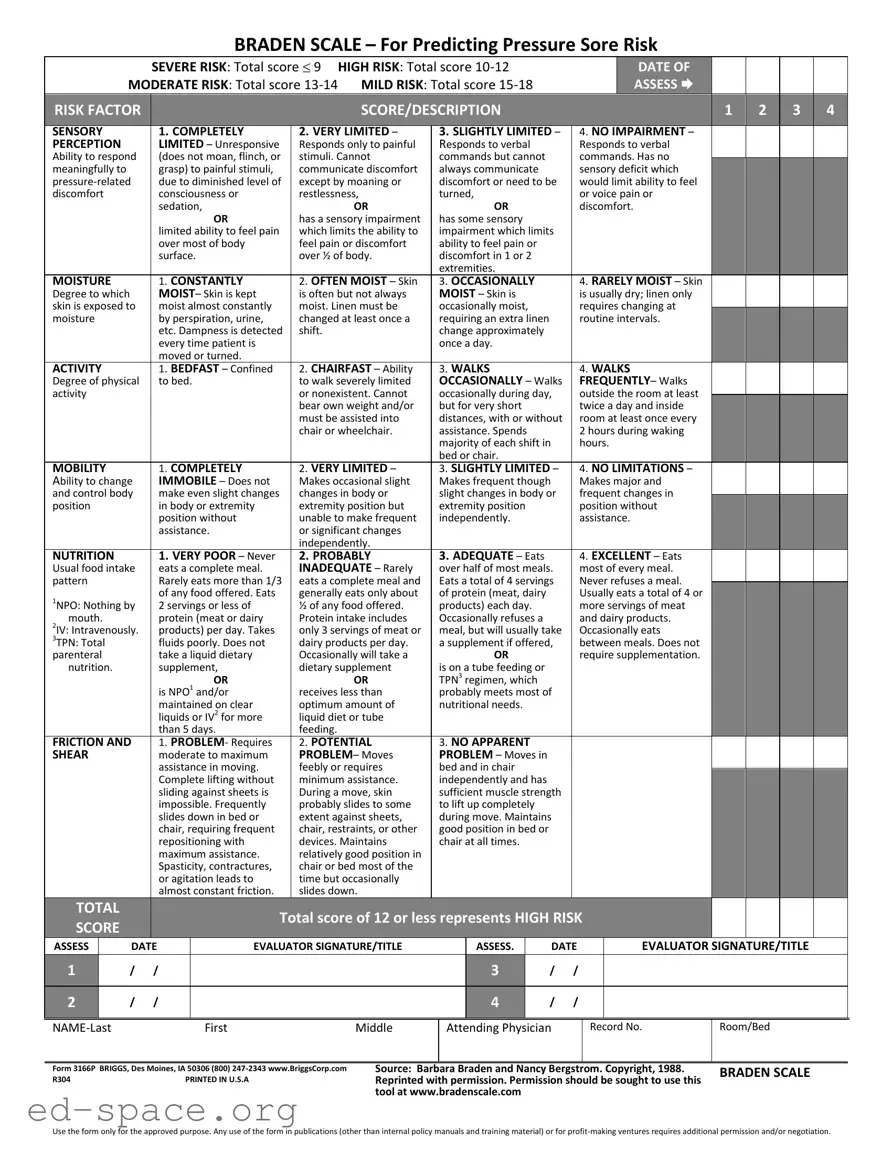
The Braden Scale is a critical tool for assessing the risk of pressure sores in patients, particularly those with limited mobility or chronic health conditions. This scale evaluates six key factors: sensory perception, moisture, activity, mobility, nutrition, and friction and shear. Each factor is assigned a score ranging from one to four, with lower scores indicating higher risk. For instance, a total score of nine signifies severe risk, while a score between ten and twelve indicates high risk. Conversely, scores from thirteen to fourteen reflect moderate risk, and scores from fifteen to eighteen suggest mild risk. The form not only facilitates a structured assessment but also helps healthcare providers implement timely interventions to prevent pressure ulcers. The Braden Scale's effectiveness hinges on the accurate evaluation of each risk factor, ensuring that patients receive appropriate care based on their individual needs. Understanding and utilizing this scale is essential for improving patient outcomes and enhancing the quality of care in various healthcare settings.
BRADEN SCALE – For Predicting Pressure Sore Risk
|
SEVERE RISK: Total score 9 |
HIGH RISK: Total score |
DATE OF |
|
MODERATE RISK: Total score |
MILD RISK: Total score |
ASSESS |
|
|
|
|
|
|
|
|
|
RISK FACTOR |
|
|
|
|
|
SCORE/DESCRIPTION |
|
|
|
|
|
|
|
1 |
2 |
3 |
4 |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SENSORY |
|
|
|
1. COMPLETELY |
2. VERY LIMITED – |
3. SLIGHTLY LIMITED – |
|
4. NO IMPAIRMENT – |
|
|
|
|||||||||||
|
|
PERCEPTION |
|
|
|
LIMITED – Unresponsive |
Responds only to painful |
Responds to verbal |
|
|
Responds to verbal |
|
|
|
||||||||||
|
|
Ability to respond |
|
|
(does not moan, flinch, or |
stimuli. Cannot |
commands but cannot |
|
|
commands. Has no |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
meaningfully to |
|
|
|
grasp) to painful stimuli, |
communicate discomfort |
always communicate |
|
|
sensory deficit which |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
due to diminished level of |
except by moaning or |
discomfort or need to be |
|
would limit ability to feel |
|
|
|
|
||||||||||||
|
|
discomfort |
|
|
|
consciousness or |
restlessness, |
turned, |
|
|
or voice pain or |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
sedation, |
OR |
|
OR |
|
|
discomfort. |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
OR |
has a sensory impairment |
has some sensory |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
limited ability to feel pain |
which limits the ability to |
impairment which limits |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
over most of body |
feel pain or discomfort |
ability to feel pain or |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
surface. |
over ½ of body. |
discomfort in 1 or 2 |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
extremities. |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
MOISTURE |
|
|
|
1. CONSTANTLY |
2. OFTEN MOIST – Skin |
3. OCCASIONALLY |
|
|
4. RARELY MOIST – Skin |
|
|
|
||||||||||
|
|
Degree to which |
|
|
|
MOIST– Skin is kept |
is often but not always |
MOIST – Skin is |
|
|
is usually dry; linen only |
|
|
|
||||||||||
|
|
skin is exposed to |
|
|
moist almost constantly |
moist. Linen must be |
occasionally moist, |
|
|
requires changing at |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
moisture |
|
|
|
by perspiration, urine, |
changed at least once a |
requiring an extra linen |
|
|
routine intervals. |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
etc. Dampness is detected |
shift. |
change approximately |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
every time patient is |
|
once a day. |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
moved or turned. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
ACTIVITY |
|
|
|
1. BEDFAST – Confined |
2. CHAIRFAST – Ability |
3. WALKS |
|
|
4. WALKS |
|
|
|
||||||||||
|
|
Degree of physical |
|
|
to bed. |
to walk severely limited |
OCCASIONALLY – Walks |
|
FREQUENTLY– Walks |
|
|
|
||||||||||||
|
|
activity |
|
|
|
|
|
|
or nonexistent. Cannot |
occasionally during day, |
|
outside the room at least |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
bear own weight and/or |
but for very short |
|
|
twice a day and inside |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
must be assisted into |
distances, with or without |
|
room at least once every |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
chair or wheelchair. |
assistance. Spends |
|
|
2 hours during waking |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
majority of each shift in |
|
hours. |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
bed or chair. |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
MOBILITY |
|
|
|
1. COMPLETELY |
2. VERY LIMITED – |
3. SLIGHTLY LIMITED – |
|
4. NO LIMITATIONS – |
|
|
|
|||||||||||
|
|
Ability to change |
|
|
IMMOBILE – Does not |
Makes occasional slight |
Makes frequent though |
|
Makes major and |
|
|
|
||||||||||||
|
|
and control body |
|
|
make even slight changes |
changes in body or |
slight changes in body or |
|
frequent changes in |
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
position |
|
|
|
in body or extremity |
extremity position but |
extremity position |
|
|
position without |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
position without |
unable to make frequent |
independently. |
|
|
assistance. |
|
|
|
|
||||||||
|
|
|
|
|
|
|
assistance. |
or significant changes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
independently. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NUTRITION |
|
|
|
1. VERY POOR – Never |
2. PROBABLY |
3. ADEQUATE – Eats |
|
|
4. EXCELLENT – Eats |
|
|
|
||||||||||
|
|
Usual food intake |
|
|
eats a complete meal. |
INADEQUATE – Rarely |
over half of most meals. |
|
most of every meal. |
|
|
|
||||||||||||
|
|
pattern |
|
|
|
Rarely eats more than 1/3 |
eats a complete meal and |
Eats a total of 4 servings |
|
Never refuses a meal. |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
1NPO: Nothing by |
|
|
of any food offered. Eats |
generally eats only about |
of protein (meat, dairy |
|
|
Usually eats a total of 4 or |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
2 servings or less of |
½ of any food offered. |
products) each day. |
|
|
more servings of meat |
|
|
|
|
|||||||||||
|
|
mouth. |
|
|
|
protein (meat or dairy |
Protein intake includes |
Occasionally refuses a |
|
|
and dairy products. |
|
|
|
|
|||||||||
|
|
2IV: Intravenously. |
|
|
products) per day. Takes |
only 3 servings of meat or |
meal, but will usually take |
|
Occasionally eats |
|
|
|
|
|||||||||||
|
|
3TPN: Total |
|
|
|
fluids poorly. Does not |
dairy products per day. |
a supplement if offered, |
|
between meals. Does not |
|
|
|
|
||||||||||
|
|
parenteral |
|
|
|
take a liquid dietary |
Occasionally will take a |
|
OR |
|
|
require supplementation. |
|
|
|
|
||||||||
|
|
nutrition. |
|
|
|
supplement, |
dietary supplement |
is on a tube feeding or |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
OR |
OR |
TPN3 regimen, which |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
is NPO1 and/or |
receives less than |
probably meets most of |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
maintained on clear |
optimum amount of |
nutritional needs. |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
liquids or IV2 for more |
liquid diet or tube |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
than 5 days. |
feeding. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
FRICTION AND |
|
|
1. PROBLEM- Requires |
2. POTENTIAL |
3. NO APPARENT |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
SHEAR |
|
|
|
moderate to maximum |
PROBLEM– Moves |
PROBLEM – Moves in |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
assistance in moving. |
|
feebly or requires |
bed and in chair |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Complete lifting without |
|
minimum assistance. |
independently and has |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
sliding against sheets is |
|
During a move, skin |
sufficient muscle strength |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
impossible. Frequently |
|
probably slides to some |
to lift up completely |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
slides down in bed or |
|
extent against sheets, |
during move. Maintains |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
chair, requiring frequent |
|
chair, restraints, or other |
good position in bed or |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
repositioning with |
|
devices. Maintains |
chair at all times. |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
maximum assistance. |
|
relatively good position in |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spasticity, contractures, |
|
chair or bed most of the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or agitation leads to |
|
time but occasionally |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
almost constant friction. |
|
slides down. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL |
|
|
|
|
Total score of 12 or less represents HIGH RISK |
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
SCORE |
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
ASSESS |
|
DATE |
|
EVALUATOR SIGNATURE/TITLE |
|
ASSESS. |
|
DATE |
|
EVALUATOR SIGNATURE/TITLE |
|
|||||||||||
|
1 |
|
/ |
/ |
|
|
|
|
|
3 |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
2 |
|
/ |
/ |
|
|
|
|
|
4 |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First |
Middle |
Attending Physician
Record No.
Room/Bed
Form 3166P BRIGGS, Des Moines, IA 50306 (800)
R304 |
PRINTED IN U.S.A |
Source: Barbara Braden and Nancy Bergstrom. Copyright, 1988. |
BRADEN SCALE |
Reprinted with permission. Permission should be sought to use this |
|
tool at www.bradenscale.com |
|
Use the form only for the approved purpose. Any use of the form in publications (other than internal policy manuals and training material) or for
| Fact Name | Description |
|---|---|
| Purpose | The Braden Scale assesses a patient's risk of developing pressure sores. |
| Scoring System | Scores range from 6 to 23, with lower scores indicating higher risk. |
| Risk Categories | Severe risk: 9 or less; High risk: 10-12; Moderate risk: 13-14; Mild risk: 15-18. |
| Components | The scale evaluates sensory perception, moisture, activity, mobility, nutrition, and friction/shear. |
| Scoring Criteria | Each component is scored from 1 to 4, with 1 indicating the highest risk. |
| Evaluation Frequency | Patients should be assessed regularly, especially after changes in condition. |
| Legal Use | In some states, the use of the Braden Scale is mandated by healthcare regulations. |
| Documentation | All assessments must be documented, including date, evaluator's signature, and patient details. |
| Copyright | The Braden Scale is copyrighted; permission is needed for non-internal use. |
| Source | Developed by Barbara Braden and Nancy Bergstrom in 1988. |
Filling out the Braden Scale form is an important step in assessing a patient's risk for pressure sores. This form requires careful attention to detail, as each section addresses different risk factors. Begin by gathering the necessary information about the patient and proceed through the scoring system methodically.
Once the form is completed, it can be used to identify the appropriate care and interventions necessary for the patient. Regular assessments may be needed to monitor changes in risk levels over time.
What is the Braden Scale and why is it important?
The Braden Scale is a tool used to assess a patient's risk of developing pressure sores, also known as bedsores. It evaluates six factors: sensory perception, moisture, activity, mobility, nutrition, and friction/shear. Each factor is scored, and the total score helps healthcare providers determine the level of risk. Understanding a patient's risk level is crucial for implementing preventative measures, ensuring better patient care, and reducing the occurrence of pressure sores.
How is the Braden Scale scored?
The Braden Scale uses a scoring system ranging from 6 to 23. Each of the six factors is assigned a score based on the patient's condition. Lower total scores indicate a higher risk for pressure sores. For example, a score of 9 indicates severe risk, while a score of 15-18 indicates mild risk. This scoring system allows healthcare providers to quickly assess and categorize a patient's risk level, guiding their care decisions.
Who should use the Braden Scale?
The Braden Scale is primarily used by healthcare professionals, including nurses and physicians, in various settings such as hospitals, nursing homes, and home care. It is essential for any caregiver responsible for patients who may be at risk for pressure sores, particularly those with limited mobility, poor nutrition, or sensory impairments. Training on how to use the scale effectively is recommended for accurate assessments.
How often should the Braden Scale be assessed?
Assessment frequency depends on the patient's condition and risk factors. Generally, it is recommended to assess patients at least once per shift or whenever there is a change in their condition. Regular assessments allow healthcare providers to monitor changes in risk levels and adjust care plans accordingly, ensuring timely interventions to prevent pressure sores.
What should be done if a patient is assessed as high risk?
If a patient is identified as high risk on the Braden Scale, immediate action is necessary. Care plans should include interventions such as regular repositioning, use of pressure-relieving devices, and nutritional support. Education for both staff and family members about the importance of prevention strategies is also crucial. By proactively addressing the identified risks, healthcare providers can significantly reduce the likelihood of pressure sore development.
When filling out the Braden Scale form, individuals may encounter several common mistakes that can affect the accuracy of the assessment. Below is a list of these mistakes:
Many people fail to apply the scoring criteria consistently across different categories. This inconsistency can lead to an inaccurate total score, which may misrepresent the patient's risk level.
Some evaluators may overlook specific details about the patient's condition. For example, failing to notice slight limitations in mobility or sensory perception can lead to an underestimation of risk.
Confusion about the terms used in the form can lead to errors. For instance, misunderstanding "very limited" versus "slightly limited" can significantly alter the assessment.
Environmental factors, such as the condition of the patient's bedding or the frequency of repositioning, are crucial. Neglecting these factors may result in a skewed perception of the patient's risk.
Effective communication among healthcare team members is vital. If team members do not share observations or concerns, the assessment may lack important insights.
Taking the time to thoroughly evaluate each risk factor is essential. Rushing through the assessment can lead to missed information and a less accurate score.
Patients' conditions can change over time. Failing to update the Braden Scale assessment regularly can result in outdated information that does not reflect the current risk level.
By being aware of these common mistakes, individuals can improve the accuracy of their assessments and provide better care for patients at risk of pressure sores.
The Braden Scale form is a valuable tool for assessing pressure sore risk in patients. It is often used in conjunction with other documents that help healthcare providers maintain comprehensive care. Below is a list of related forms and documents that are commonly utilized alongside the Braden Scale.
Using these documents in conjunction with the Braden Scale form enhances patient care and promotes better outcomes. Each form serves a specific purpose, contributing to a holistic approach to patient assessment and management.
The Braden Scale form is a widely used tool for assessing pressure sore risk. Several other documents share similarities with the Braden Scale in terms of purpose and structure. Here are five such documents:
When filling out the Braden Scale form, it is crucial to approach the task with care and attention to detail. Here are ten recommendations to ensure accuracy and effectiveness:
By adhering to these guidelines, the risk assessment process can be more effective, ultimately leading to better patient care.
The Braden Scale is a widely used tool for assessing the risk of pressure sores in patients. However, several misconceptions surround its use and interpretation. Here are seven common misunderstandings:
Understanding these misconceptions can enhance the effective use of the Braden Scale, ultimately improving patient care and outcomes.
Understanding the Braden Scale form is essential for assessing the risk of pressure sores. Here are some key takeaways to keep in mind:
By keeping these points in mind, healthcare providers can effectively utilize the Braden Scale to enhance patient care and minimize the risk of pressure sores.