The Biopsychosocial Assessment Social Work form serves as a comprehensive tool designed to gather essential information about an individual's mental health, social circumstances, and biological factors. This form is structured to capture a wide array of details, starting with personal identifiers such as name, date of birth, and preferred language, ensuring that each client feels recognized and understood. It delves into the presenting problem, inviting individuals to articulate their reasons for seeking help, the duration of their issues, and the impact on daily functioning. Clients are encouraged to express their therapy goals, providing a clear direction for treatment. The assessment also explores emotional and psychological symptoms, including feelings of sadness, anxiety, or suicidal thoughts, which are crucial for understanding the client's current state. Furthermore, it examines the individual's history with substances, relationships, education, legal issues, work history, and medical background, painting a holistic picture of their life circumstances. By addressing these multifaceted aspects, the form not only aids social workers in developing effective intervention strategies but also empowers clients to reflect on their experiences and aspirations for the future.

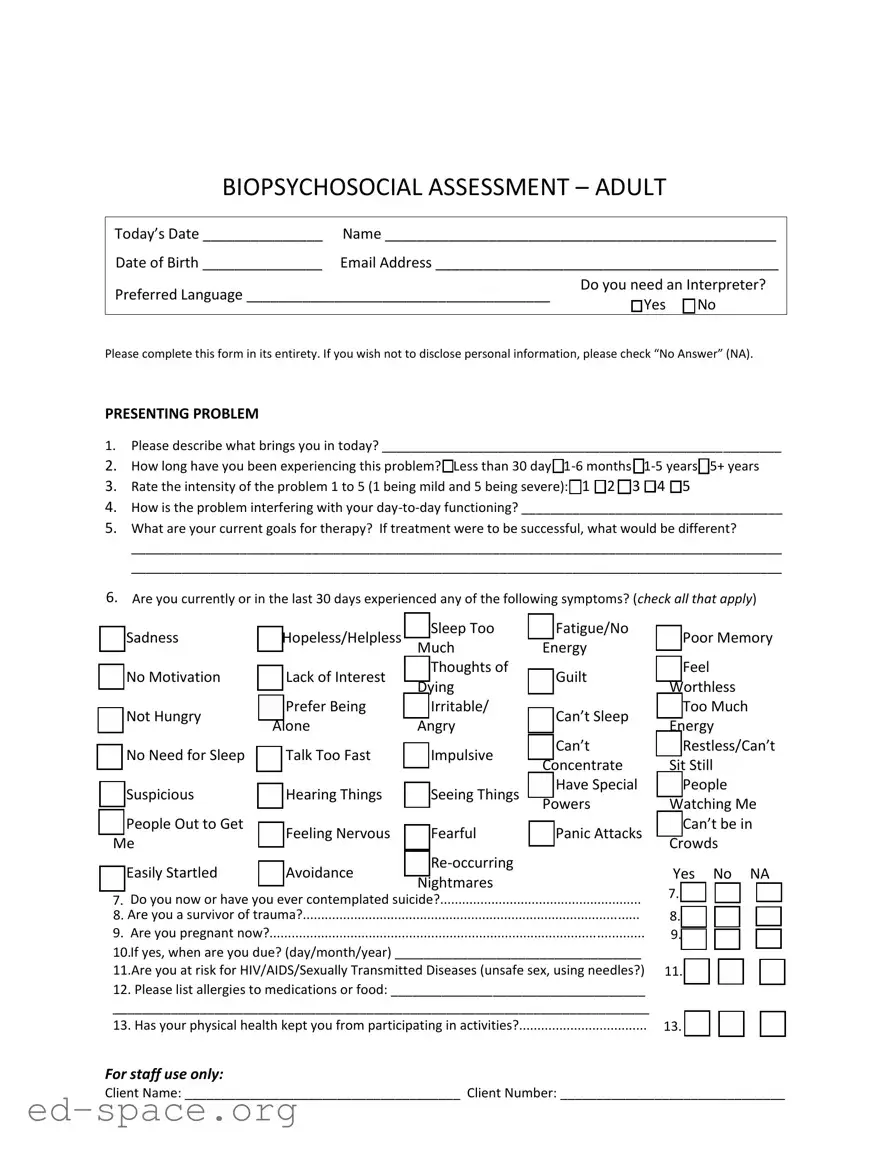
BIOPSYCHOSOCIAL ASSESSMENT – ADULT
Today’s Date _______________ |
Name _________________________________________________ |
Date of Birth _______________ |
Email Address ___________________________________________ |
Preferred Language ______________________________________ |
Do you need an Interpreter? |
|
□ Yes □ No |
||
|
Please complete this form in its entirety. If you wish not to disclose personal information, please check “No Answer” (NA).
PRESENTING PROBLEM
1.Please describe what brings you in today? _______________________________________________________
2.How long have you been experiencing this problem? □Less than 30 day
3.Rate the intensity of the problem 1 to 5 (1 being mild and 5 being severe): □1 □2 □3 □4 □5
4.How is the problem interfering with your
5.What are your current goals for therapy? If treatment were to be successful, what would be different?
__________________________________________________________________________________________
__________________________________________________________________________________________
6.Are you currently or in the last 30 days experienced any of the following symptoms? (check all that apply)
□Sadness
□No Motivation
□Not Hungry
□No Need for Sleep
□Suspicious
□People Out to Get
Me
□Easily Startled
□Hopeless/Helpless |
□ Sleep Too |
□ Fatigue/No |
|
|
Much |
Energy |
|
□ Lack of Interest |
□ Thoughts of |
□ Guilt |
|
Dying |
|||
|
|
||
□ Prefer Being |
□ Irritable/ |
□ Can’t Sleep |
|
Alone |
Angry |
||
|
|||
□ Talk Too Fast |
□ Impulsive |
□ Can’t |
|
Concentrate |
|||
|
|
||
□ Hearing Things |
□ Seeing Things |
□ Have Special |
|
Powers |
|||
|
|
||
□ Feeling Nervous |
□ Fearful |
□ Panic Attacks |
|
□ Avoidance |
□ |
|
|
Nightmares |
|
||
|
|
□Poor Memory
□Feel
Worthless
□Too Much
Energy
□Restless/Can’t
Sit Still
□People
Watching Me
□Can’t be in Crowds
Yes No NA |
7. Do you now or have you ever contemplated suicide?.......................................................
8. Are you a survivor of trauma?............................................................................................
9. Are you pregnant now?......................................................................................................
10.If yes, when are you due? (day/month/year) __________________________________
11.Are you at risk for HIV/AIDS/Sexually Transmitted Diseases (unsafe sex, using needles?)
12. Please list allergies to medications or food: ___________________________________
__________________________________________________________________________
13. Has your physical health kept you from participating in activities?...................................
7. |
□ |
□ |
□ |
8. |
□ |
□ |
□ |
9. |
□ |
□ |
□ |
11. |
□ |
□ |
□ |
13. |
□ |
□ |
□ |
For staff use only:
Client Name: ______________________________________ Client Number: _______________________________
TOBACCO |
|
Yes |
No |
NA |
1. Have you ever used any forms of tobacco (cigarettes, snuff, etc.)? IF NO SKIP TO NEXT |
1. |
□ |
□ |
□ |
SECTION……………………………………………………………………………………………………………………………… |
|
|
|
|
2. Are you a former tobacco user? |
2. |
□ |
□ |
□ |
3.If yes, what form(s) of tobacco have you used in the past (please check all that apply)
□ Cigarettes □ Cigars □ Snuff □ Chewing Tobacco □ Snuff □ Other
4.How many times on an average day do you use tobacco
Cigarettes____ Cigars____ Snuff____ Chewing Tobacco____ Snuff____ |
|
|
|
|
5. Have you been involved in a program to help you quit using tobacco in the past 30 |
5. |
□ |
□ |
□ |
days? |
|
|
|
|
6. If so, which |
|
|
|
|
SUBSTANCE USE/ADDICTION PRESENT |
|
Yes |
No |
NA |
1. Would you or someone you know say you are having a problem with alcohol?......………… |
1. |
□ |
□ |
□ |
2. Would you or someone you know say you are having problems with pills or illegal |
2. |
□ |
□ |
□ |
drugs? |
|
|
|
|
3. Would you or someone you know say you are having problems with other addictions, ie. |
3. |
□ |
□ |
□ |
gambling, pornography or shopping? |
|
|
|
|
4. Have you ever been to a |
4. |
□ |
□ |
□ |
SUBSTANCE USE/ADDICTION PAST |
|
Yes |
No |
NA |
1. Would you or someone you know say you had a problem with alcohol?......…………………… |
1. |
□ |
□ |
□ |
2. Would you or someone you know say you had problems with pills or illegal drugs? |
2. |
□ |
□ |
□ |
3. Would you or someone you know say you had problems with other addictions, ie. |
3. |
□ |
□ |
□ |
gambling, pornography or shopping? |
|
|
|
|
4. Is there a family history of addiction in your family? |
4. |
□ |
□ |
□ |
5. If yes, please describe: _____________________________________________________ |
|
|
|
|
PERSONAL, FAMILY AND RELATIONSHIPS |
|
Yes |
No |
NA |
1.Who is in your family? (parents, brothers, sisters, children, etc.)____________________
__________________________________________________________________________
2. |
Has there been any significant person or family member enter or leave your life in the |
2. □ |
□ |
□ |
|||||
last 90 days? |
|
|
|
|
|
|
|||
|
|
Good Fair Poor Close Stressful Distant Other |
|||||||
3. |
How are the relationships in your family? |
□ |
□ |
□ |
□ |
□ |
□ |
□ |
|
4. |
How are the relationships in your support system (friends, |
□ |
□ |
□ |
□ |
□ |
□ |
□ |
|
extended family, et.?)………………………………………………………………. |
|||||||||
|
|
|
|
|
|
|
|||
|
|
|
|
Conflict Abuse Stress Loss Other |
|||||
5. |
Are there any problems in your family now? (check all that apply)………….. |
□ |
□ |
□ |
□ |
□ |
|||
6. |
Were there any problems with your family in the past? (check all that |
|
□ |
□ |
□ |
□ |
□ |
||
apply)…………………………………………………………………………………………………………... |
|
|
|
|
|
||||
7. Are there any problems in your support system now? (check all that |
|
□ |
□ |
□ |
□ |
□ |
|||
apply)…………………………………………………………………………………………………………… |
|
|
|
|
|
||||
8. Were there any problems with your support system in the past? (check |
□ |
□ |
□ |
□ |
□ |
||||
all that apply)………………………………………………………………………………………………. |
|
|
|
|
|
||||
9.What is your marital status now? □Single □Married □Living as Married □Divorced □Widowed □Never Married
For staff use only:
Client Name: ______________________________________ Client Number: _______________________________
10.Have you ever had problems with marriage/relationships?..............................................
11.If yes, please check why: □Stress □Conflict □Loss □Divorced/Separation
□Trust Issues □Other_______________________________
12.Do you have any close friends?..........................................................................................
13.Do you have problems with friendships?...........................................................................
14.Do you get along well with others (neighbors,
15.What do you like to do for fun? _____________________________________________
Yes |
No |
NA |
10. □ |
□ |
□ |
12. □ |
□ |
□ |
13. □ |
□ |
□ |
14. □ |
□ |
□ |
EDUCATION
1.What is the highest grad you completed in school? (please check)
□No Education
2.Would you describe your school experience as positive or negative?________________
3.Are you currently in school or a training program?..............................................................
Yes No NA
3. □ □ |
□ |
LEGAL
1.Have you ever been arrested? IF NO SKIP TO NEXT SECTION………………………………………….
2.In the past month?...............................................................................................................
3.If yes, how many times? ____________________________________________________
4.In the past year?...................................................................................................................
5.If yes, how many times? ____________________________________________________
6.If yes, what were you arrested for? ___________________________________________
7.What was the name of your attorney? ________________________________________
8.Were you ever sentenced for a crime?…………………………………………………………………………….
9.If yes, number of prison sentences served? ____________________________________
10.What year(s) did this occur? _______________________________________________
11.Are you currently or have you ever been on probation or parole?....................................
12.If yes, what is the name of your attorney or probation officer? ____________________
WORK
1.What is your work history like? □Good □Poor □Sporadic □Other
2.How long do you normally keep a job? □Weeks □Months □Years
3.Are you retired?....................................................................................................................
4.If yes, what kind of work do you do/did you do in the past? _______________________
5.Have you ever served in the military?..................................................................................
6.If yes, are you: □Active □Retired □Other
|
Yes |
No |
NA |
1. |
□ |
□ |
□ |
2. |
□ |
□ |
□ |
4. |
□ |
□ |
□ |
8. |
□ |
□ |
□ |
11. □ |
□ |
□ |
|
|
Yes |
No |
NA |
3. |
□ |
□ |
□ |
5. |
□ |
□ |
□ |
MEDICAL
1.Current Primary Care Physician: __________________________________Phone_________________
2.Past and Current Medical/Surgical Problems: _____________________________________________
3.Past and Current Medications and Dosages: ______________________________________________
__________________________________________________________________________________
4. Have you seen a Mental Health Professional Before? □ Yes □ No
5.If yes, Name, When, and Reason for Changing: ____________________________________________
6.Current Psychiatrist/APRN, if applicable:_________________________________________________
7.Is there anything else you would like me to know about you?_______________________________
__________________________________________________________________________________
For staff use only:
Client Name: ______________________________________ Client Number: _______________________________
| Fact Name | Fact Description |
|---|---|
| Purpose | The Biopsychosocial Assessment form is designed to gather comprehensive information about an individual's psychological, social, and biological factors affecting their well-being. |
| Client Information | It collects essential client details such as name, date of birth, email address, and preferred language, ensuring effective communication and service delivery. |
| Presenting Problem | The form prompts clients to describe their main issue, duration of the problem, and its impact on daily life, facilitating targeted support. |
| Symptom Checklist | Clients can indicate current symptoms, including feelings of sadness or anxiety, which helps in identifying urgent needs and areas for intervention. |
| Substance Use | The assessment includes sections on current and past substance use, which is crucial for understanding addiction issues and formulating treatment plans. |
| Family and Relationships | It explores family dynamics and relationships, helping to identify potential support systems or conflicts that may affect treatment. |
| Legal History | The form asks about any legal issues, including arrests, which can impact a client's mental health and treatment options. |
| Governing Laws | The assessment is governed by state-specific laws related to mental health services, ensuring compliance with regulations such as HIPAA for privacy and confidentiality. |
Completing the Biopsychosocial Assessment Social Work form is an important step in understanding your needs and goals. This form gathers vital information that will help guide your therapy and support. Take your time to fill it out thoroughly, as it will provide valuable insights into your current situation and history.
What is the purpose of the Biopsychosocial Assessment Social Work form?
The Biopsychosocial Assessment form is designed to gather comprehensive information about an individual's mental, emotional, and physical health. It helps social workers understand a person's presenting problems, personal history, family dynamics, and social environment. This information is crucial for developing an effective treatment plan tailored to the individual's needs.
How should I complete the form if I don't want to disclose certain information?
If there are sections of the form that you prefer not to answer, you can simply check the “No Answer” (NA) option. Your comfort and privacy are important, and it's perfectly acceptable to skip questions that you feel are too personal or sensitive. The goal is to provide as much or as little information as you feel comfortable sharing.
What types of questions can I expect on the form?
The form includes a variety of questions covering several areas of your life. You will be asked about your current problems, symptoms, family relationships, education, legal history, and work experience. There are also questions about your medical history and any past mental health treatment. This holistic approach ensures that all aspects of your life are considered in your assessment.
What happens after I submit the Biopsychosocial Assessment form?
Once you submit the form, a social worker will review your responses. They may reach out to you for clarification or additional information if needed. This assessment will help them understand your situation better and create a personalized plan to support you. Your input is invaluable in this process, and it sets the foundation for your future sessions.
Failing to provide complete personal information, such as name or date of birth, can delay processing.
Not specifying the preferred language or the need for an interpreter may lead to communication issues during sessions.
Omitting details about the presenting problem can hinder the understanding of the situation.
Choosing vague options for the duration of the problem, such as "1-6 months," without providing additional context can create confusion.
Failing to rate the intensity of the problem accurately may affect treatment planning.
Not checking all applicable symptoms in the symptom checklist can lead to an incomplete assessment of mental health.
Neglecting to disclose any history of suicidal thoughts can be a significant oversight in understanding risk factors.
Overlooking questions about family relationships and support systems may result in missing crucial contextual information.
Failing to provide information about substance use or past addictions can lead to inadequate support strategies.
Not mentioning any legal issues or past arrests can affect the overall assessment of the individual’s situation.
The Biopsychosocial Assessment Social Work form is a critical tool used in social work practice to gather comprehensive information about a client's mental, physical, and social well-being. However, it is often accompanied by various other forms and documents that enhance the assessment process and provide a more holistic view of the client's situation. Below is a list of related documents frequently utilized in conjunction with the Biopsychosocial Assessment.
These documents, when used alongside the Biopsychosocial Assessment, create a robust framework for understanding and addressing the complexities of a client's life. Together, they enhance the social worker's ability to provide effective and tailored support to those in need.
When filling out the Biopsychosocial Assessment Social Work form, keep the following tips in mind:
There are several misconceptions about the Biopsychosocial Assessment Social Work form that can lead to misunderstandings about its purpose and use. Here are six common misconceptions:
Filling out the Biopsychosocial Assessment Social Work form is an important step in the therapeutic process. Here are some key takeaways to keep in mind: