The Application For Driver form is a crucial document for anyone seeking employment as a commercial driver. This form is designed to gather essential information about an applicant's background, including personal details, driving experience, and employment history. Carriers must ensure that the form is filled out completely, as incomplete applications will not be considered. Key sections of the form include the applicant's contact information, residency history, and a declaration of legal eligibility to work in the United States. Additionally, it requires a detailed account of the applicant's driving licenses, accident records, and traffic violations over the past three years. The form also emphasizes the importance of listing all relevant employment history for the last ten years, particularly focusing on any positions subject to Federal Motor Carrier Safety Regulations. Lastly, it includes a section for the applicant to authorize background checks and verify the accuracy of the information provided. This comprehensive approach ensures that carriers can make informed hiring decisions while adhering to regulatory requirements.
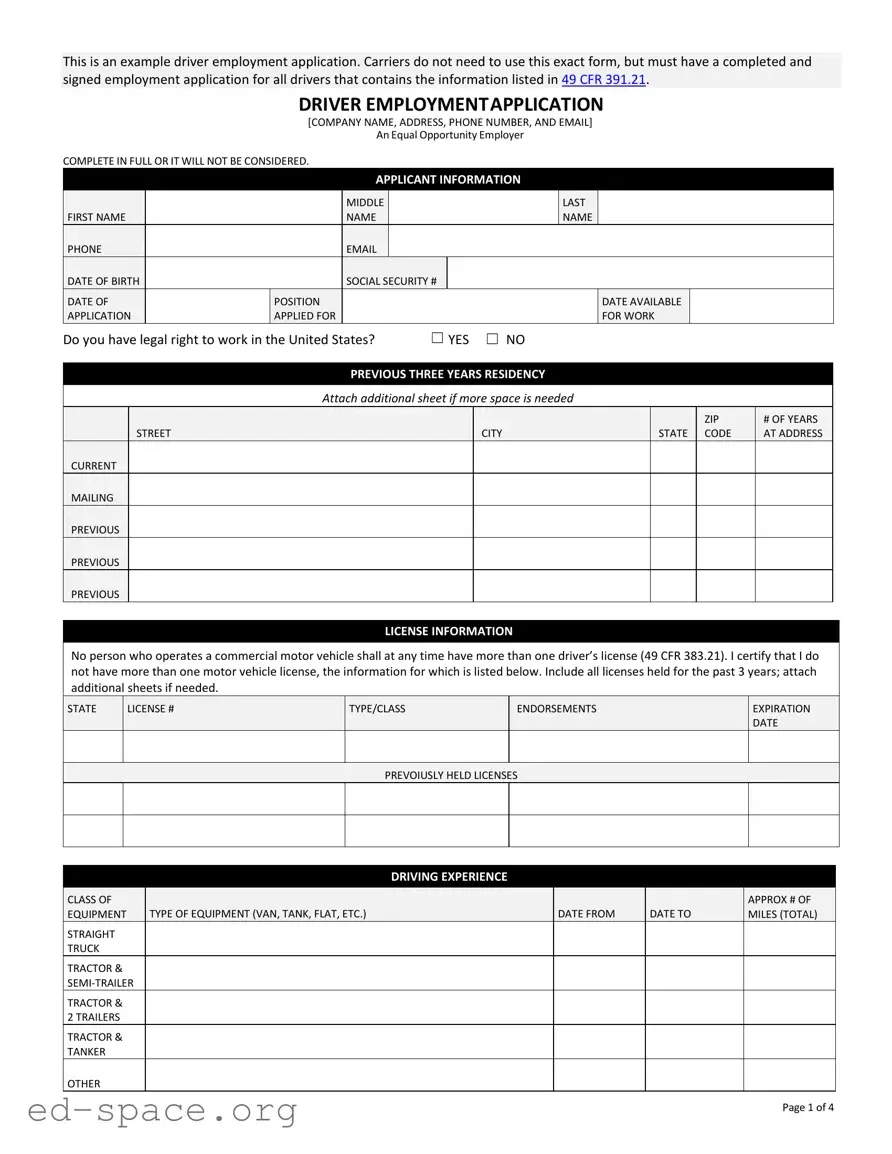
This is an example driver employment application. Carriers do not need to use this exact form, but must have a completed and signed employment application for all drivers that contains the information listed in 49 CFR 391.21.
DRIVER EMPLOYMENTAPPLICATION
[COMPANY NAME, ADDRESS, PHONE NUMBER, AND EMAIL]
An Equal Opportunity Employer
COMPLETE IN FULL OR IT WILL NOT BE CONSIDERED.
|
|
|
|
APPLICANT INFORMATION |
|
|
|
|
|
|
|||
|
|
|
|
MIDDLE |
|
|
|
LAST |
|
|
|
|
|
FIRST NAME |
|
|
NAME |
|
|
|
NAME |
|
|
|
|
|
|
PHONE |
|
|
|
|
|
|
|
|
|
|
|
||
DATE OF BIRTH |
|
|
SOCIAL SECURITY # |
|
|
|
|
|
|
|
|
||
DATE OF |
|
POSITION |
|
|
|
|
|
DATE AVAILABLE |
|
|
|
||
APPLICATION |
|
APPLIED FOR |
|
|
|
|
|
FOR WORK |
|
|
|
||
Do you have legal right to work in the United States? |
☐ YES ☐ NO |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PREVIOUS THREE YEARS RESIDENCY |
|
|
|
|
|
|
|||
|
|
|
Attach additional sheet if more space is needed |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
ZIP |
# OF YEARS |
|
STREET |
|
|
|
|
CITY |
|
|
STATE |
|
CODE |
AT ADDRESS |
|
CURRENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
MAILING |
|
|
|
|
|
|
|
|
|
|
|
|
|
PREVIOUS |
|
|
|
|
|
|
|
|
|
|
|
|
|
PREVIOUS |
|
|
|
|
|
|
|
|
|
|
|
|
|
PREVIOUS |
|
|
|
|
|
|
|
|
|
|
|
|
|
LICENSE INFORMATION
No person who operates a commercial motor vehicle shall at any time have more than one driver’s license (49 CFR 383.21). I certify that I do not have more than one motor vehicle license, the information for which is listed below. Include all licenses held for the past 3 years; attach additional sheets if needed.
STATE
LICENSE #
TYPE/CLASS
ENDORSEMENTS
EXPIRATION DATE
PREVOIUSLY HELD LICENSES
DRIVING EXPERIENCE
CLASS OF |
|
TYPE OF EQUIPMENT (VAN, TANK, FLAT, ETC.) |
|
DATE FROM |
|
DATE TO |
APPROX # OF |
EQUIPMENT |
|
|
|
MILES (TOTAL) |
|||
STRAIGHT |
|
|
|
|
|
|
|
TRUCK |
|
|
|
|
|
|
|
TRACTOR & |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TRACTOR & |
|
|
|
|
|
|
|
2 TRAILERS |
|
|
|
|
|
|
|
TRACTOR & |
|
|
|
|
|
|
|
TANKER |
|
|
|
|
|
|
|
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 1 of 4 |
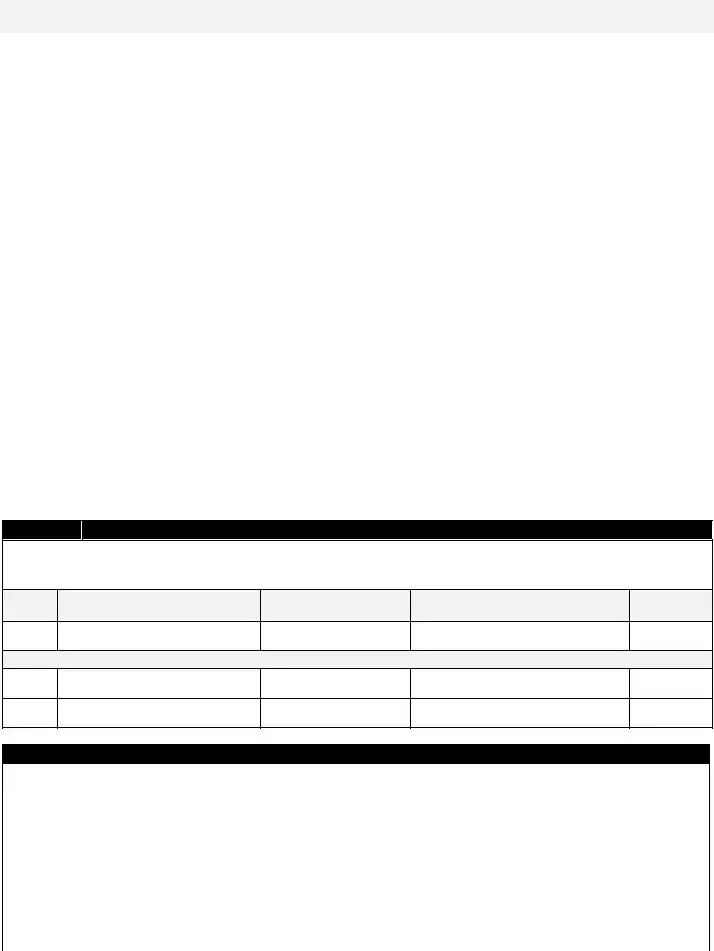
ACCIDENT RECORD FOR THE PAST 3 YEARS
Attach additional sheet if more space is needed. Check this box if none ☐
DATES (List most recent first)
NATURE OF ACCIDENT
CHEMICAL SPILLS
# FATALITIES # INJURIES (Y/N)
TRAFFIC CONVICTIONS AND FORFEITURES FOR THE PAST 3 YEARS (OTHER THAN PARKING VIOLATIONS)
Attach additional sheet if more space is needed. Check this box if none ☐
DATE CONVICTED (Month/Year)
VIOLATION
STATE OF
VIOLATION PENALTY (Forfeited bond, collateral and/or points)
Have you ever been denied a license, permit, or privilege to operate a motor vehicle? |
☐ YES |
☐ NO |
If yes, explain |
|
|
Has any license, permit, or privilege ever been suspended or revoked? |
☐ YES |
☐ NO |
If yes, explain |
|
|
EMPLOYMENT HISTORYZ
The Federal Motor Carrier Safety Regulations (49 CFR 391.21) require that all applicants wishing to drive a commercial vehicle list all employment for the last three (3) years. In addition, if you have driven a commercial vehicle previously, you must provide employment history for an additional seven (7) years (for a total of ten (10) years). Any gaps in employment in excess of one (1) month must be explained.
Start with the last or current position, including any military experience, and work backwards (attach separate sheets if necessary). You are required to list the complete mailing address, including street number, city, state, zip; and complete all other information.
CURRENT (MOST RECENT) EMPLOYER |
|
|
|
|
|
|
|||
NAME |
|
|
|
|
|
PHONE |
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
|
|
|
TO |
|
POSITION HELD |
|
|
MO/YR |
|
|
|
MO/YR |
|
|
REASON FOR LEAVING |
|
|
|
|
|
SALARY |
|
||
EXPLAIN ANY GAPS IN |
|
|
|
|
|
|
|
||
EMPLOYMENT (Include |
|
|
|
|
|
|
|
||
month/year & reason) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
Page 2 of 4 |

While employed here, were you subject to the Federal Motor Carrier Safety Regulations? |
|
|
|
|
☐ YES |
☐ NO |
|
|||||||||||
Was the job designated as a |
|
|
|
|
|
|
||||||||||||
mode subject to alcohol and controlled substances testing as required by 49 CFR, part 40? |
|
|
|
|
☐ YES |
☐ NO |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECOND (MOST RECENT) EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
NAME |
|
|
|
|
|
|
|
|
PHONE |
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
|
|
TO |
|
|
|
|
|
|
||
POSITION HELD |
|
|
|
|
MO/YR |
|
|
MO/YR |
|
|
|
|
|
|
||||
REASON FOR LEAVING |
|
|
|
|
|
|
|
SALARY |
|
|
|
|
|
|||||
EXPLAIN ANY GAPS IN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
EMPLOYMENT (Include |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
month/year & reason) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
While employed here, were you subject to the Federal Motor Carrier Safety Regulations? |
|
|
|
|
☐ YES |
☐ NO |
||||||||||||
Was the job designated as a |
|
|
|
|
|
|
||||||||||||
mode subject to alcohol and controlled substances testing as required by 49 CFR, part 40? |
|
|
|
|
☐ YES |
☐ NO |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
THIRD (MOST RECENT) EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
NAME |
|
|
|
|
|
|
|
|
PHONE |
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
|
|
TO |
|
|
|
|
|
|
||
POSITION HELD |
|
|
|
|
MO/YR |
|
|
MO/YR |
|
|
|
|
|
|
||||
REASON FOR LEAVING |
|
|
|
|
|
|
|
SALARY |
|
|
|
|
|
|||||
EXPLAIN ANY GAPS IN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
EMPLOYMENT (Include |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
month/year & reason) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
While employed here, were you subject to the Federal Motor Carrier Safety Regulations? |
|
|
|
|
☐ YES |
☐ NO |
|
|||||||||||
Was the job designated as a |
|
|
|
|
|
|
||||||||||||
mode subject to alcohol and controlled substances testing as required by 49 CFR, part 40? |
|
|
|
|
☐ YES |
☐ NO |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
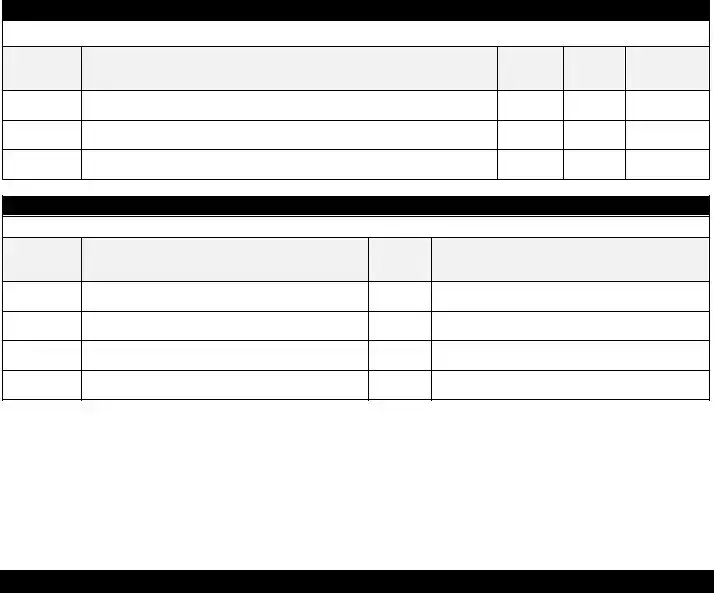
EDUCATION |
|
|
|
|
|
|
|
|
|
||||
SCHOOL |
|
NAME & LOCATION |
|
|
COURSE OF STUDY |
YEARS |
GRADUATE |
DETAILS |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
COMPLETED |
Y |
N |
|
|
|
|
||
High School |
|
|
|
|
|
|
|
|
☐ |
|
☐ |
|
|
|
|
|||
College |
|
|
|
|
|
|
|
|
☐ |
|
☐ |
|
|
|
|
|||
Other |
|
|
|
|
|
|
|
|
☐ |
|
☐ |
|
|
|
|
|||
OTHER QUALIFICATIONS
Please list any other qualifications that you have and which you believe should be considered.
Page 3 of 4
TO BE READ AND SIGNED BY APPLICANT
I authorize you to make investigations (including contacting current and prior employers) into my personal, employment, financial, medical history, and other related matters as may be necessary in arriving at an employment decision. I hereby release employers, schools, health care providers, and other persons from all liability in responding to inquiries and releasing information in connection with my application.
In the event of employment, I understand that false or misleading information given in my application or interview(s) may result in discharge. I also understand that I am required to abide by all rules and regulations of the Company.
I understand that the information I provide regarding my current and/or prior employers may be used, and those employer(s) will be contacted for the purpose of investigating my safety performance history as required by 49 CFR 391.23. I understand that I have the right to:
•Review information provided by current/previous employers;
•Have errors in the information corrected by previous employers, and for those previous employers to resend the corrected information to the prospective employer; and
•Have a rebuttal statement attached to the alleged erroneous information, if the previous employer(s) and I cannot agree on the accuracy of the information.
This certifies that I completed this application, and that all entries on it and information in it are true and complete to the best of my knowledge. Note: A motor carrier may require an applicant to provide more information than that required by the Federal Motor Carrier Safety Regulations.
Applicant Signature
Applicant Name (printed)
Date
Page 4 of 4
| Fact Name | Description |
|---|---|
| Governing Law | The application must comply with 49 CFR 391.21, which outlines the requirements for driver employment applications. |
| Equal Opportunity Employer | The form states that the employer is an Equal Opportunity Employer, promoting non-discrimination in hiring practices. |
| Completion Requirement | Applicants must complete the form in full; incomplete applications will not be considered. |
| Residency Disclosure | Applicants are required to provide their residency history for the past three years, including addresses and duration at each location. |
| License Information | Applicants must declare all driver's licenses held in the past three years, adhering to the stipulation of having only one active license (49 CFR 383.21). |
| Accident Record | Applicants need to disclose any accidents from the past three years, including details such as nature of the accident and any fatalities or injuries. |
| Employment History | The form requires a detailed employment history for the last three years, with additional information needed for the previous seven years if applicable. |
Completing the Application for Driver form is an essential step in the hiring process for drivers. This form gathers necessary information about the applicant's background, driving history, and qualifications. Once the form is filled out, it will be submitted to the employer for review, along with any required supporting documents.
What is the purpose of the Application For Driver form?
The Application For Driver form is used by carriers to gather necessary information from applicants seeking employment as drivers. It ensures that all required details are collected, as mandated by federal regulations. This includes personal information, driving history, and previous employment records.
What information do I need to provide on the form?
You must complete the form in full, providing details such as your name, contact information, date of birth, Social Security number, and employment history for the past ten years. Additionally, you will need to disclose your driving experience, accident record, and any traffic violations. If applicable, include information about your education and other qualifications.
Can I use a different form instead of the one provided?
What happens if I do not complete the form fully?
If the form is not completed in full, it will not be considered for employment. It is essential to provide all requested information to avoid delays or disqualification from the application process.
What should I do if I have gaps in my employment history?
You need to explain any gaps in employment that exceed one month. Include the month and year of the gap along with the reason for it. This transparency helps employers understand your work history better.
What rights do I have regarding the information I provide?
You have the right to review the information provided by your current and previous employers. If you find errors, you can request corrections. If there is a disagreement about the accuracy of the information, you can attach a rebuttal statement to the records.
Not providing complete contact information. Applicants often leave out their phone number or email address, which can hinder communication.
Failing to list all previous employment. Many applicants forget to include jobs held in the last three years or do not provide details for positions held longer than that.
Inaccurate or incomplete license information. Some applicants do not include all licenses held in the past three years or fail to mention expired licenses.
Omitting gaps in employment. When there are breaks in work history, applicants often neglect to explain these gaps, which can raise questions.
Not signing the application. Some applicants forget to provide their signature at the end of the form, which is required for the application to be valid.
When applying for a driver position, several forms and documents are commonly required alongside the Application for Driver form. These documents help ensure that the application process is thorough and compliant with regulations.
These documents collectively support the application process and help employers make informed hiring decisions. Ensuring that all required forms are completed accurately and submitted in a timely manner can streamline the hiring process.
Things to Do When Filling Out the Application For Driver Form:
Things to Avoid When Filling Out the Application For Driver Form:
Misconception 1: The Application for Driver form is mandatory for all carriers.
In reality, while the form provides a useful template, carriers are not required to use it. They must, however, have a completed and signed employment application that includes the necessary information as outlined in the regulations.
Misconception 2: Applicants can skip sections if they find them irrelevant.
This is not true. The form must be completed in full. Missing information may result in the application not being considered. Every section serves a purpose in evaluating the applicant's qualifications and history.
Misconception 3: Previous employment history is not important if there are gaps.
On the contrary, any gaps in employment exceeding one month must be explained. This requirement helps employers understand an applicant's work history and any potential issues that may arise from extended periods of unemployment.
Misconception 4: The application process does not involve background checks.
This is a common misunderstanding. The form includes a section where applicants authorize investigations into their personal and employment history. Employers are allowed to contact previous employers to assess the applicant's safety performance history.
Completing the Application For Driver form is a critical step in the hiring process for commercial drivers. Here are some key takeaways to ensure the application is filled out accurately and effectively:
By following these guidelines, applicants can enhance their chances of a successful application process. Thoroughness and honesty are paramount in presenting qualifications for a driving position.