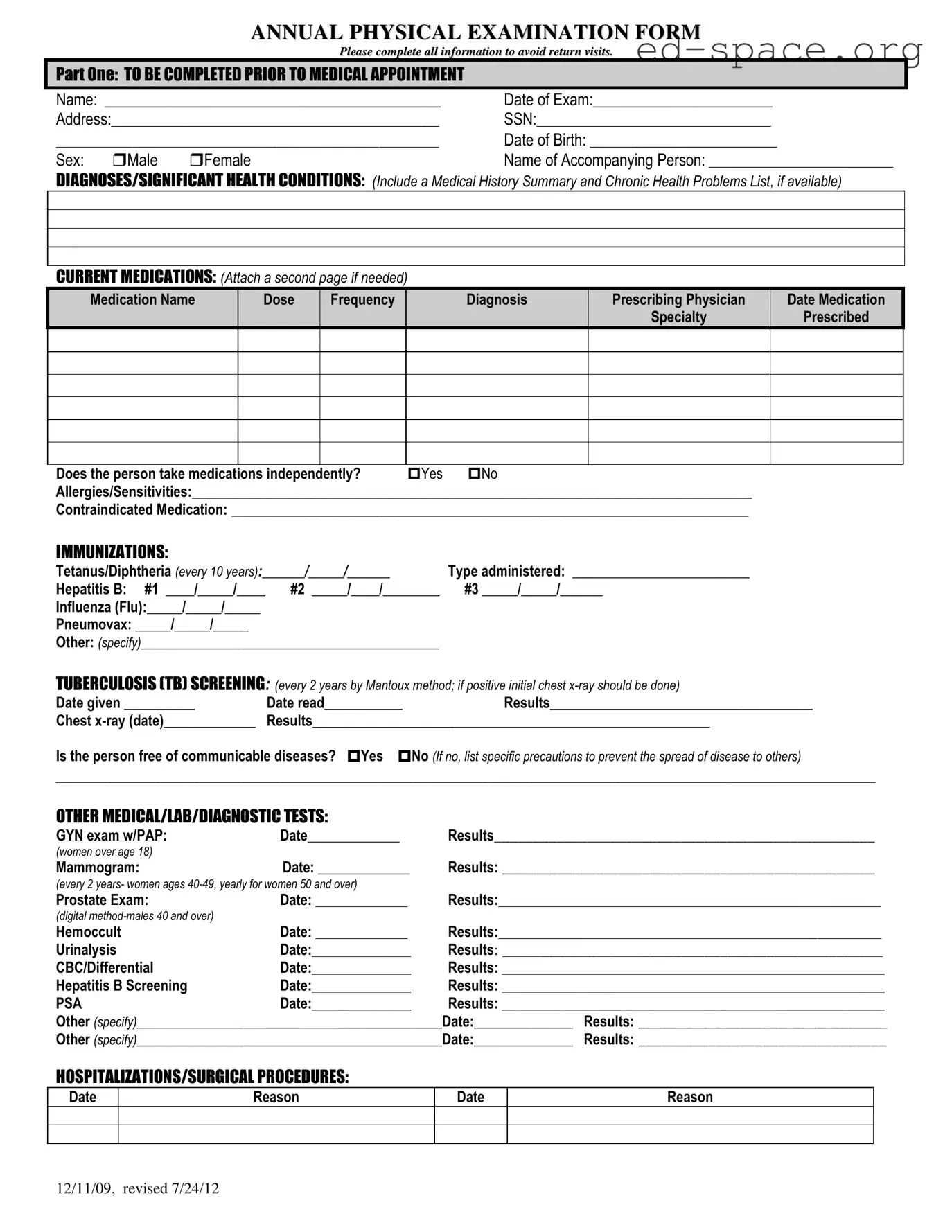
The Annual Physical Examination form serves as an essential document that systematically captures a comprehensive range of health-related information. Designed to minimize the need for return visits, it requires the completion of all sections, spanning from personal identification details like name, date of birth, social security number, and address to the more intricate health-related information. This includes a detailed medical history, any significant health conditions, current medications, known allergies or sensitivities, immunization records, and results from previous medical, lab, or diagnostic tests. Part one of the form is primarily geared towards gathering baseline health data, while part two delves into the specifics of the physical examination, evaluating various systems within the body such as cardiovascular, respiratory, gastrointestinal, and more, to ensure a thorough health review. Furthermore, it encompasses records related to vision and hearing screening, hospitalizations, surgical procedures, and imposes queries about any changes in health status from the previous year, ultimately guiding health maintenance recommendations, identifying any limitations or restrictions, and suggesting further evaluations by specialists if needed. The meticulous design of the form aims to facilitate a detailed health overview, thereby assisting healthcare providers in delivering tailored care and making informed decisions.

| Fact | Description |
|---|---|
| 1. Form Revision Dates | The form has been revised twice, on December 11, 2009, and July 24, 2012. |
| 2. Comprehensive Personal Details | Includes sections for personal information such as Name, SSN, Date of Birth, and Address. |
| 3. Accompanying Person | There's a provision to mention the name of a person accompanying the individual to the medical appointment. |
| 4. Detailed Medical History | Requires a summary of diagnoses/significant health conditions, chronic health problems list, and current medications. |
| 5. Immunization Record | Documents immunization history, including Tetanus/Diphtheria, Hepatitis B, Influenza, Pneumococcal vaccines, and others. |
| 6. TB Screening | Mandates tuberculosis screening every 2 years using the Mantoux method and subsequent actions if the initial test is positive. |
| 7. Screening and Diagnostic Tests | Includes records for various tests such as GYN exam, Mammogram, Prostate Exam, Hemoccult, Urinalysis, CBC/Differential, Hepatitis B Screening, and PSA among others specified. |
| 8. Hospitalization and Surgical Procedures | Contains a section for listing hospitalizations and surgical procedures with dates and reasons. |
| 9. General Physical Examination Components | Details the evaluation of systems including blood pressure, pulse, respirations, and a review of bodily systems. |
| 10. Recommendations and Limitations | Provides space for recommendations regarding health maintenance, limitations or restrictions for activities, use of adaptive equipment, and changes in health status. |
Filling out the Annual Physical Examination form thoroughly is essential for ensuring comprehensive health care. This form is designed to record vital health information, medical history, and examination results. By accurately completing this form, patients and healthcare providers can ensure a well-documented health profile that aids in preventive care and medical management. The following steps are designed to help patients, or their accompanying persons, complete the form efficiently and accurately.
By following these steps, you will provide a comprehensive health overview that facilitates proper medical care and support. Remember to review all entered information for accuracy before submitting the form to your healthcare provider.
What information is needed to fill out the Annual Physical Examination form?
To complete the Annual Physical Examination form correctly, it requires an array of detailed information. Firstly, personal identification details such as name, date of the exam, address, Social Security Number (SSN), date of birth, and sex need to be filled out. You should also provide the name of any accompanying person. The health-related sections call for a comprehensive medical history including diagnoses/significant health conditions, a list of current medications specifying each medication's name, dose, frequency, prescribing physician, and the date it was prescribed. It also requires information on whether medications are taken independently, any allergies or medications that are contraindicated, immunization records, TB screening results, and results of other medical, lab, or diagnostic tests. The form further asks about hospitalizations/surgical procedures, general physical exam results including blood pressure and temperature, an evaluation of various body systems, and details regarding vision and hearing screening. Finally, it solicits information on health maintenance recommendations, any limitations or restrictions for activities, the use of any adaptive equipment, changes in health status, and recommendations for specialty consults.
How often should TB screening be done according to the form?
According to the Annual Physical Examination form, TB (Tuberculosis) screening should be conducted every 2 years. This screening is recommended to be performed using the Mantoux method. If the initial screening results are positive, a chest x-ray should be done to further assess the individual's health status regarding TB.
Are there specific guidelines for women's health screening mentioned in the form?
Yes, the form outlines specific health screening guidelines for women. It mentions that women over the age of 18 should have a GYN exam with a PAP smear. Meanwhile, mammograms are recommended every 2 years for women aged 40-49 and yearly for women aged 50 and over. These screenings are important parts of preventative health measures for women, helping to detect potential issues early.
What should you do if you need more space for the medication section?
If you find that the current medications section on the form does not provide enough space for your needs, you are encouraged to attach a second page to list all medications adequately. This ensures that your health care provider has a comprehensive understanding of your current medications, including the names, dosages, frequencies, diagnoses, prescribing physicians, and dates prescribed. Providing complete information is crucial for accurate medical review and care.
Filling out an Annual Physical Examination form is a critical step in ensuring you receive accurate medical care and advice. However, mistakes can be made that may impact the completeness and reliability of the provided information. Here are six common pitfalls to avoid:
Not updating personal information. It’s important to ensure that details such as address, phone number, and emergency contact information are current. Changes in these areas can affect how quickly you or your loved ones are contacted in case of a medical issue.
Leaving the medication section incomplete. All medications, including over-the-counter drugs, vitamins, and supplements, should be listed along with their dosages and frequency. This helps in identifying possible drug interactions and assessing your overall treatment plan.
Forgetting to mention allergies or sensitivities. It is crucial to list all known allergies, especially to medications, to avoid potentially dangerous reactions during or after the examination process.
Not providing a comprehensive medical history. Including prior and chronic health conditions, surgeries, hospitalizations, and any significant family medical history gives a clearer picture of your overall health and potential risk factors.
Omitting information on lifestyle habits. Details regarding smoking, alcohol consumption, exercise, and diet can greatly influence recommendations for health maintenance or adjustments in treatment plans.
Failure to review and sign the form. A signed form not only verifies that the information provided is accurate to the best of your knowledge but also authorizes the healthcare provider to proceed with the examination and necessary treatments based on the recorded information.
When approaching your Annual Physical Examination form, take the time to review each section carefully. Ensuring the completeness and accuracy of every field can significantly enhance the quality of care you receive and prevent unnecessary follow-up visits or clarifications.
When navigating healthcare, particularly for a thorough annual physical examination, various forms and documents complement the Annual Physical Examination form to ensure comprehensive care and record-keeping. These additional documents are vital for a well-rounded understanding and evaluation of an individual's health status.
These documents, when used in conjunction with the Annual Physical Examination form, provide a comprehensive view of an individual's health, facilitating informed medical decisions and proactive health management. Each document plays a pivotal role in ensuring that the care provided is both accurate and aligned with the patient's unique health needs and preferences.
The Annual Physical Examination form shares similarities with a Medical History Questionnaire. Both documents collect comprehensive health-related information from the patient, including past diagnoses, medical conditions, and a summary of the patient’s medical history. They serve as essential tools for healthcare providers to understand the patient’s health background before making any current assessments or treatment plans.
A Medication Management Record parallels the Annual Physical Examination form in its objective to document all current medications that a patient is taking, along with dosage, frequency, and prescribing physician. This ensures a holistic view of the patient's treatment regimen, allows for the monitoring of potential drug interactions, and assists in evaluating the efficacy of current medications.
Similar to an Immunization Record, the Annual Physical Examination form includes sections dedicated to recording the patient's immunization status. Both documents track vaccinations received, including the type of vaccine administered and the date, which is critical for preventing vaccine-preventable diseases and ensuring the patient is up to date with recommended immunizations.
The examination form also resembles a Laboratory and Diagnostic Test Results Record, as it succinctly documents past tests, screenings, and their outcomes. Like a specialized record, it encompasses a wide range of tests from hemoccult to urinalysis and mammograms, providing a snapshot of the patient’s recent and relevant test results which contribute to diagnosing and monitoring health conditions.
When completing the Annual Physical Examination form, it's vital to approach the task with careful attention to detail and thoroughness. To ensure the process is approached correctly, here are some essential do's and don'ts:
Do:There are several common misconceptions about the Annual Physical Examination form that can lead to confusion. Understanding these can help in properly completing the form and ensuring a comprehensive check-up. Here are six misconceptions and the explanations behind them:
Correcting these misconceptions and ensuring the form is filled out accurately and comprehensively can significantly enhance the effectiveness of the Annual Physical Examination, aiding in better health management and care.
Filling out the Annual Physical Examination Form thoroughly and accurately is crucial. Here are four key takeaways to ensure the process is completed efficiently:
By following these guidelines, individuals and healthcare professionals can work together more effectively to manage and maintain health.
What Is a Medevac Flight - It includes a checklist to ensure all necessary information is provided before submission.
Hazmat Bill of Lading - The clear structure of the form allows for straightforward completion and review by employers.