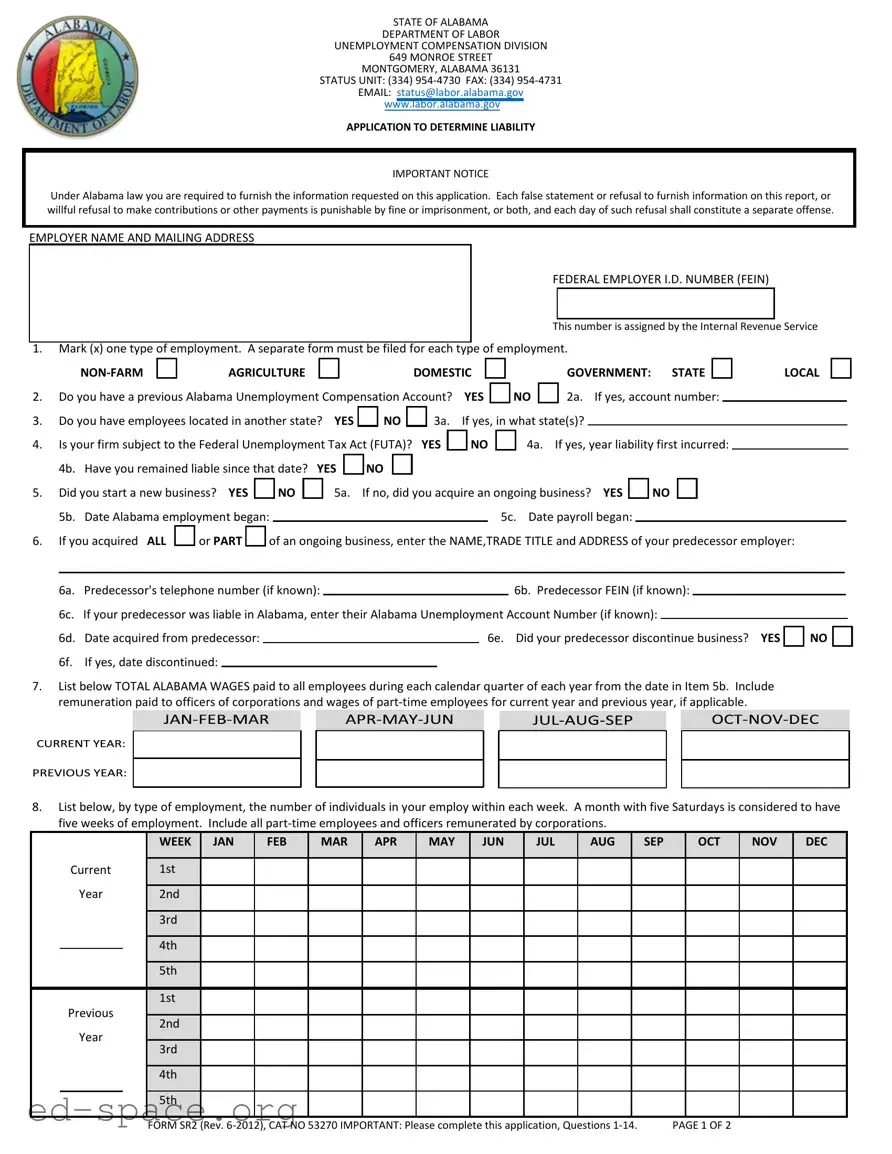
The Alabama Sr 2 form is a crucial document for employers seeking to determine their liability under the state's unemployment compensation laws. This application, issued by the Alabama Department of Labor, requires detailed information about the employer's business structure, employee count, and payroll history. Employers must provide their name, mailing address, and federal employer identification number, along with specific details about their type of employment—whether it be non-farm, agriculture, or domestic. The form also inquires about any previous unemployment accounts, the existence of employees in other states, and the applicability of the Federal Unemployment Tax Act. Additionally, employers must disclose their total Alabama wages and the number of individuals employed during each week of the year. Completing this form accurately is essential, as any false statements or refusal to provide requested information can lead to penalties, including fines or imprisonment. By following the instructions carefully and submitting all required information, employers can ensure compliance with Alabama's unemployment compensation regulations.
STATE OF ALABAMA
DEPARTMENT OF LABOR
UNEMPLOYMENT COMPENSATION DIVISION
649 MONROE STREET
MONTGOMERY, ALABAMA 36131
STATUS UNIT: (334)
EMAIL: [email protected]
www.labor.alabama.gov
APPLICATION TO DETERMINE LIABILITY
IMPORTANT NOTICE
Under Alabama law you are required to furnish the information requested on this application. Each false statement or refusal to furnish information on this report, or willful refusal to make contributions or other payments is punishable by fine or imprisonment, or both, and each day of such refusal shall constitute a separate offense.
EMPLOYER NAME AND MAILING ADDRESS
FEDERAL EMPLOYER I.D. NUMBER (FEIN)
This number is assigned by the Internal Revenue Service
1.Mark (x) one type of employment. A separate form must be filed for each type of employment.
AGRICULTURE |
DOMESTIC |
|
GOVERNMENT: STATE |
LOCAL |
|
2. Do you have a previous Alabama Unemployment Compensation Account? YES |
NO |
2a. If yes, account number: |
|
||
3. Do you have employees located in another state? YES |
NO |
4.Is your firm subject to the Federal Unemployment Tax Act (FUTA)?
3a. If yes, in what state(s)?
YES |
NO |
4a. If yes, year liability first incurred: |
|
4b. |
Have you remained liable since that date? |
YES |
NO |
|
|
|
||||||
5. |
Did you start a new business? YES |
|
NO |
|
5a. |
If no, did you acquire an ongoing business? YES |
NO |
||||||
|
5b. |
Date Alabama employment began: |
|
|
|
|
5c. Date payroll began: |
|
|
|
|||
6. |
If you acquired ALL |
or PART |
of an ongoing business, enter the NAME,TRADE TITLE and ADDRESS of your predecessor employer: |
||||||||||
|
|
|
|
|
|
|
|
|
|||||
|
6a. |
Predecessor's telephone number (if known): |
|
|
|
6b. Predecessor FEIN (if known): |
|
|
|||||
6c. If your predecessor was liable in Alabama, enter their Alabama Unemployment Account Number (if known):
6d. Date acquired from predecessor:
6f. If yes, date discontinued:
6e. Did your predecessor discontinue business? YES |
NO |
7.List below TOTAL ALABAMA WAGES paid to all employees during each calendar quarter of each year from the date in Item 5b. Include remuneration paid to officers of corporations and wages of
8.List below, by type of employment, the number of individuals in your employ within each week. A month with five Saturdays is considered to have five weeks of employment. Include all
|
|
|
|
WEEK |
JAN |
|
MAR |
APR |
|
JUN |
JUL |
|
|
SEP |
|
OCT |
NOV |
DEC |
|
|
|
|
|
FEB |
MAY |
AUG |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Current |
|
1st |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2nd |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3rd |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4th |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5th |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Previous |
|
1st |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
2nd |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
3rd |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4th |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5th |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
FORM SR2 |
(Rev. |
|
PAGE 1 OF 2 |
|
|
|||||||||||
9.ITEM 9 MUST BE COMPLETED IN ITS ENTIRETY. Use the enclosed instruction sheet for Item 9 to complete Columns
|
Column |
Column |
Column |
Column |
Column |
Name |
1 |
2 |
3 |
4 |
5 |
Location |
|
|
|
|
|
|
Name and location |
Alabama |
Employee |
Indicate specific type of activity in detail |
Enter |
|
Enter "Statewide" if no permanent location |
County |
count per |
See Instructions Sheet for Assistance |
Percent |
|
|
unit |
|
|
|
|
|
|
|
|
% |
|
|
|
|
|
% |
|
|
|
|
|
% |
%
9a. |
Is the above work site primarily engaged in performing support or services for other work sites of the company? YES |
NO |
||||||||||
9b. |
To whom are most of your products sold? GENERAL PUBLIC |
CONSTRUCTION CONTRACTORS |
RETAILERS |
|
|
|
||||||
|
WHOLESALERS |
OTHERS |
(Specify) |
|
|
|
|
|
|
|
|
|
10. Form of organization: INDIVIDUAL |
PARTNERSHIP |
CORPORATION |
ASSOCIATION |
ESTATE OR TRUST |
LLC (see 10a.) |
|||||||
OTHER |
(Specify) |
|
|
|
|
|
|
|
||||
10a. Indicate tax filing status with IRS (include all members and their social security numbers or Federal Identification numbers in Item 11)
CORPORATION |
PARTNERSHIP |
SOLE PROPRIETOR |
DISREGARDED ENTITY |
|
10b. Is the organization exempt under 501(c)(3) of the IRS Code? YES |
NO |
(If yes, submit a copy of the 501(c)(3) letter of exemption.) |
||
11. For positive identification, list below the full name(s), social security number(s) and title(s) of individual owner, partners or officers.
Name
Social Security Number
Title
12. |
If not otherwise subject, do you wish to voluntarily elect coverage under the Alabama Law? YES |
NO |
|
13. |
Name and business location/physical address: |
13a. Tax Preparer/CPA/Accountant: |
|
Name of Applicant, Employer, Corporation, Partnership, Trust, etc.
Trade Name or Division (if different from above)
Physical Address
City |
County |
State |
Zip |
|
|
|
|
Area Code – Telephone |
|
Area Code – Facsimile |
|
|
|
|
|
Contact Person |
|
|
|
|
|
|
|
Email Address |
|
|
|
Name of Tax Preparer/CPA/Accountant
Trade Name or Division (if different from above)
Address
City |
County |
State |
Zip |
|
|
|
|
Area Code – Telephone |
|
Area Code – Facsimile |
|
|
|
|
|
Contact Person |
|
|
|
|
|
|
|
Email Address |
|
|
|
I certify the information provided on this application is true and correct to the best of my knowledge.
14. Business Name:Signature:Date:
NOTE: IF CPA, TAX PREPARER, ETC., IS ONLY SIGNATURE, PLEASE ENCLOSE POWER OF ATTORNEY.
FORM SR2 (Rev. |
PAGE 2 OF 2 |
| Fact Name | Fact Detail |
|---|---|
| Governing Law | Alabama Code Title 25, Chapter 4 governs unemployment compensation. |
| Form Purpose | The SR 2 form is used to determine employer liability for unemployment compensation. |
| Filing Requirement | Employers must complete this application to provide necessary information. |
| False Statements | Providing false information can result in fines or imprisonment. |
| Account Number | Employers with a previous account must provide their Alabama Unemployment Compensation Account number. |
| Employment Types | Employers must mark the type of employment: non-farm, agriculture, or domestic. |
| New Business | Questions are included to determine if the employer is starting a new business or acquiring an ongoing one. |
| Wage Reporting | Employers must report total Alabama wages paid to employees for each quarter. |
Filling out the Alabama SR 2 form is an important step for employers looking to determine their unemployment compensation liability. Once you have completed the form, you will submit it to the Alabama Department of Labor to ensure compliance with state regulations. Here’s how to fill it out step by step:
After completing these steps, double-check your entries for accuracy. Once everything is in order, submit the form to the Alabama Department of Labor. This will help you stay compliant and avoid any potential issues down the line.
What is the Alabama SR 2 form?
The Alabama SR 2 form is an application used to determine liability for unemployment compensation in Alabama. Employers must complete this form to provide essential information regarding their business operations and employee counts. It is a critical step in ensuring compliance with Alabama's unemployment laws.
Who needs to fill out the Alabama SR 2 form?
What information is required on the form?
What happens if false information is provided?
How do I determine my unemployment account number?
What if I have employees in multiple states?
Is there a deadline for submitting the Alabama SR 2 form?
Can I get help filling out the Alabama SR 2 form?
What should I do after completing the form?
When filling out the Alabama SR 2 form, individuals often make several common mistakes that can lead to delays or complications in processing their applications. Here are four mistakes to watch out for:
Many applicants fail to provide accurate details regarding their employer name and mailing address. This information is crucial for the processing of your application. Double-check for typos or incorrect addresses that could lead to miscommunication.
It is essential to answer all questions completely. Skipping questions, especially those regarding previous unemployment accounts or employee locations, can result in a rejection of your application. Ensure that you provide thorough responses to each item.
Applicants often misreport total Alabama wages paid to employees. This section requires accurate figures for each calendar quarter. Failing to include all remuneration, or miscalculating amounts, can lead to discrepancies that complicate your application.
One of the simplest yet most common errors is neglecting to sign and date the form. Without a signature, the application is incomplete and cannot be processed. Always review the form before submission to ensure it is fully signed.
By being aware of these common pitfalls, applicants can improve their chances of a smooth and efficient application process.
The Alabama Sr 2 form is a critical document for employers seeking to determine their unemployment compensation liability. However, it is often accompanied by several other forms and documents that help facilitate the process. Understanding these additional documents can ensure compliance and streamline the filing process. Below is a list of commonly used forms and documents alongside the Alabama Sr 2 form.
In summary, the Alabama Sr 2 form serves as a foundational document for employers navigating unemployment compensation. However, the accompanying forms and documents are equally important, as they contribute to a comprehensive understanding of employment obligations and compliance requirements. Properly managing these documents can facilitate a smoother process for both employers and employees.
When filling out the Alabama SR 2 form, there are several important dos and don’ts to keep in mind. Following these guidelines can help ensure your application is processed smoothly.
By following these guidelines, you can help ensure that your application is complete and accurate, reducing the chances of delays or issues in processing.
Misconceptions about the Alabama Sr 2 form can lead to confusion for employers. Here are five common misunderstandings:
Understanding these points can help ensure compliance and avoid unnecessary complications when dealing with unemployment compensation in Alabama.
When filling out and using the Alabama SR 2 form, there are several important points to consider:
By following these key takeaways, you can ensure that your application is complete and accurate, facilitating a smoother process for determining your liability under Alabama unemployment compensation laws.