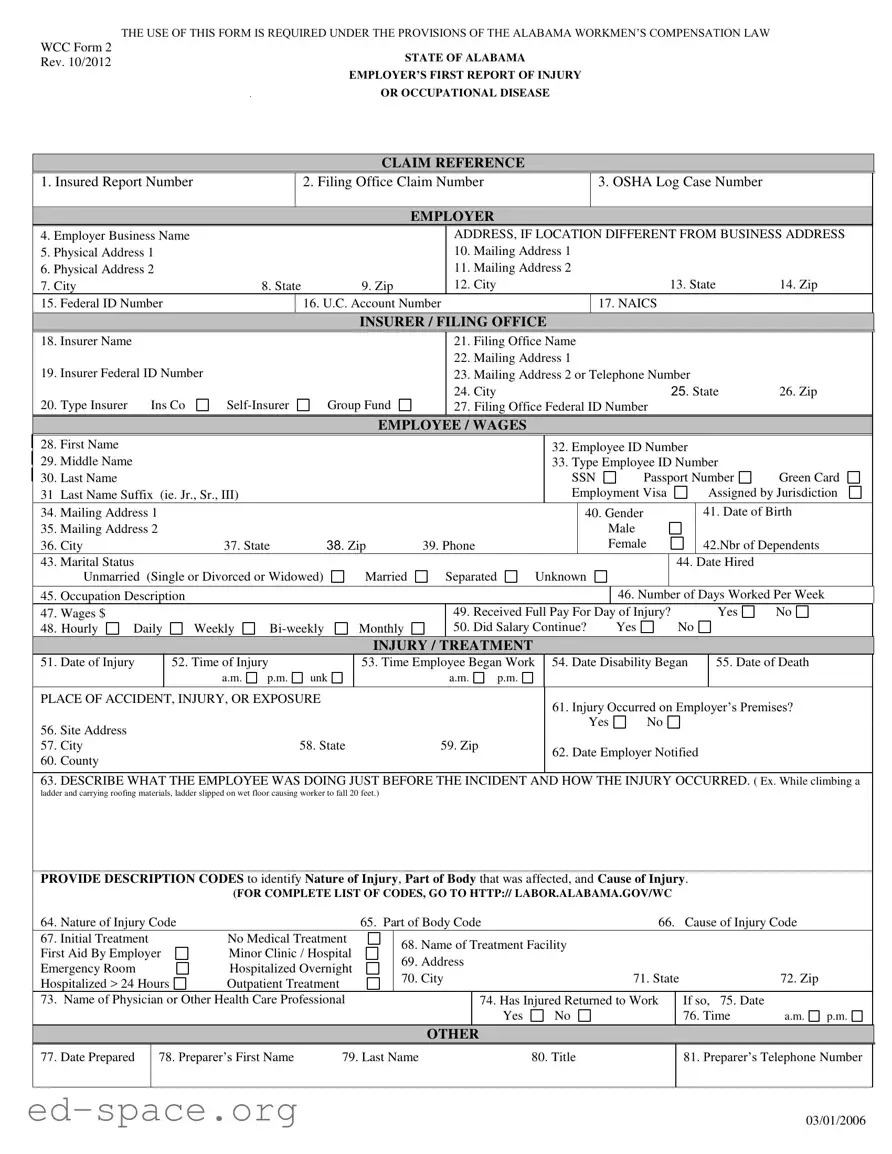
The Alabama First Report form is a critical document in the realm of workers' compensation, designed to streamline the reporting process for injuries or occupational diseases that occur in the workplace. This form, mandated by the Alabama Workmen’s Compensation Law, serves as the employer's official notification to the relevant authorities regarding an employee's injury. It collects essential information, including the employer's details, the injured employee's personal information, and specifics about the incident itself. Key sections of the form require the reporting of the date and time of the injury, the nature of the injury, and the treatment received. Additionally, it includes codes to categorize the type of injury, the affected body part, and the cause of the injury, which aids in statistical tracking and analysis. The form also prompts the employer to provide information about the employee's wages and employment status, ensuring a comprehensive overview of the circumstances surrounding the incident. By completing this form accurately and promptly, employers fulfill their legal obligations while also facilitating the necessary support for injured workers.
THE USE OF THIS FORM IS REQUIRED UNDER THE PROVISIONS OF THE ALABAMA WORKMEN’S COMPENSATION LAW
WCC Form 2
Rev. 10/2012STATE OF ALABAMA
EMPLOYER’S FIRST REPORT OF INJURY
OR OCCUPATIONAL DISEASE
CLAIM REFERENCE
|
|
1. Insured Report Number |
|
|
2. Filing Office Claim Number |
|
|
|
|
|
3. OSHA Log Case Number |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. Employer Business Name |
|
|
|
|
|
|
ADDRESS, IF LOCATION DIFFERENT FROM BUSINESS ADDRESS |
|
|||||||||||||||||
|
|
5. Physical Address 1 |
|
|
|
|
|
|
|
|
10. Mailing Address 1 |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
6. Physical Address 2 |
|
|
|
|
|
|
|
|
11. Mailing Address 2 |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
7. City |
|
|
|
|
8. State |
|
9. Zip |
|
12. City |
|
|
|
|
|
|
|
|
13. State |
14. Zip |
|
|||||
|
|
15. Federal ID Number |
|
|
16. U.C. Account Number |
|
|
|
|
|
17. NAICS |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
INSURER / FILING OFFICE |
|
|
|
|
|
|
|
|
|
|
||||||
|
18. |
Insurer Name |
|
|
|
|
|
|
|
|
|
21. Filing Office Name |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
22. Mailing Address 1 |
|
|
|
|
|
|
|
|
|
|
||||
|
19. |
Insurer Federal ID Number |
|
|
|
|
|
23. Mailing Address 2 or Telephone Number |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
24. City |
|
|
|
|
|
|
|
|
25. State |
26. Zip |
|
|||
|
20. |
Type Insurer |
Ins Co |
|
Group Fund |
|
27. Filing Office Federal ID Number |
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
EMPLOYEE / WAGES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
28. First Name |
|
|
|
|
|
|
|
|
|
|
|
|
32. Employee ID Number |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
29. Middle Name |
|
|
|
|
|
|
|
|
|
|
|
|
33. Type Employee ID Number |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
30. |
Last Name |
|
|
|
|
|
|
|
|
|
|
|
|
SSN |
Passport Number |
Green Card |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
31 |
Last Name Suffix |
(ie. Jr., Sr., III) |
|
|
|
|
|
|
|
|
Employment Visa |
|
Assigned by Jurisdiction |
|
||||||||||||
|
34. |
Mailing Address 1 |
|
|
|
|
|
|
|
|
|
|
|
|
40. Gender |
|
|
|
41. Date of Birth |
|
|||||||
|
35. |
Mailing Address 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
|
|
|
|||
|
36. |
City |
|
|
|
37. State |
|
38. Zip |
39. Phone |
|
|
|
|
|
Female |
|
42.Nbr of Dependents |
|
|||||||||
|
43. |
Marital Status |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
44. Date Hired |
|
|
|||||
|
|
|
Unmarried (Single or Divorced or Widowed) |
|
Married |
|
Separated |
|
Unknown |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
45. |
Occupation Description |
|
|
|
|
|
|
|
|
|
|
|
|
|
46. Number of Days Worked Per Week |
|
||||||||||
|
47. |
Wages $ |
|
|
|
|
|
|
|
|
|
49. Received Full Pay For Day of Injury? |
|
Yes |
No |
|
|||||||||||
|
|
48. Hourly |
Daily |
Weekly |
|
Monthly |
|
50. Did Salary Continue? |
|
|
Yes |
|
No |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
INJURY / TREATMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
51. |
Date of Injury |
|
52. Time of Injury |
|
|
53. Time Employee Began Work |
|
54. Date Disability Began |
|
55. Date of Death |
|
|||||||||||||||
|
|
|
|
|
|
|
a.m. |
p.m. |
unk |
|
|
a.m. |
p.m. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
PLACE OF ACCIDENT, INJURY, OR EXPOSURE |
|
|
|
|
|
|
61. Injury Occurred on Employer’s Premises? |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
56. |
Site Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
57. |
City |
|
|
|
|
|
58. State |
59. Zip |
|
|
62. Date Employer Notified |
|
|
|
|
|||||||||||
|
60. |
County |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
63. DESCRIBE WHAT THE EMPLOYEE WAS DOING JUST BEFORE THE INCIDENT AND HOW THE INJURY OCCURRED. ( Ex. While climbing a
ladder and carrying roofing materials, ladder slipped on wet floor causing worker to fall 20 feet.)
PROVIDE DESCRIPTION CODES to identify Nature of Injury, Part of Body that was affected, and Cause of Injury.
|
(FOR COMPLETE LIST OF CODES, GO TO HTTP:// LABOR.ALABAMA.GOV/WC |
|
|
||||||
64. Nature of Injury Code |
|
65. Part of Body Code |
66. |
|
Cause of Injury Code |
||||
67. Initial Treatment |
No Medical Treatment |
|
68. |
Name of Treatment Facility |
|
|
|||
First Aid By Employer |
Minor Clinic / Hospital |
|
|
|
|||||
|
69. |
Address |
|
|
|
|
|||
Emergency Room |
Hospitalized Overnight |
|
|
|
|
|
|||
|
70. |
City |
71. State |
|
72. Zip |
||||
Hospitalized > 24 Hours |
Outpatient Treatment |
|
|
||||||
|
|
|
|
|
|
|
|
||
73. Name of Physician or Other Health Care Professional |
|
|
|
74. Has Injured Returned to Work |
|
If so, 75. Date |
|
||
|
|
|
|
|
Yes |
No |
|
76. Time |
a.m. p.m. |
|
|
|
|
|
|
|
|
|
|
OTHER
77. Date Prepared
78. Preparer’s First Name |
79. Last Name |
80. Title |
81. Preparer’s Telephone Number
03/01/2006
| Fact Name | Details |
|---|---|
| Governing Law | The Alabama First Report form is governed by the Alabama Workmen’s Compensation Law. |
| Form Purpose | This form is required for reporting injuries or occupational diseases to ensure compliance with state regulations. |
| Form Revision Date | The current version of the form is WCC Form 2, revised in October 2012. |
| Employer Information | Employers must provide their business name, physical address, and mailing address if different. |
| Employee Identification | Key employee details include name, Social Security Number, and employment status. |
| Injury Details | Specifics about the injury, including date, time, and circumstances, must be clearly described. |
| Insurance Information | Insurers must be identified, including their name, type, and federal ID number. |
| Filing Office | Information regarding the filing office, including name and address, is also required. |
| Return to Work | The form includes a section to indicate whether the injured employee has returned to work. |
Completing the Alabama First Report form is essential for reporting workplace injuries or occupational diseases. After filling out the form, it must be submitted to the appropriate filing office. The following steps will guide you through the process of accurately completing the form.
What is the Alabama First Report form and why is it necessary?
The Alabama First Report form is a document required under the Alabama Workmen’s Compensation Law. It serves as an official report of an injury or occupational disease that occurs in the workplace. This form must be completed by the employer and submitted to the appropriate insurance provider or filing office. Its primary purpose is to ensure that injured employees receive the necessary benefits and medical treatment in a timely manner. Completing this form accurately and promptly is crucial for both the employer and the employee to navigate the workers' compensation process effectively.
Who is responsible for filling out the Alabama First Report form?
The responsibility of filling out the Alabama First Report form falls on the employer. The employer must provide detailed information about the incident, including the employee's personal details, the nature of the injury, and the circumstances surrounding the event. It is essential for employers to gather accurate information from the injured employee and any witnesses to ensure the report reflects the true nature of the incident. Failure to complete the form correctly can lead to delays in benefits for the injured worker.
What information is required on the Alabama First Report form?
The Alabama First Report form requires comprehensive information about the employer, the injured employee, and the specifics of the incident. Key details include the employer's business name and address, the employee's name, Social Security Number, and occupation. Additionally, the form asks for the date and time of the injury, a description of what the employee was doing before the injury occurred, and the type of medical treatment received. The form also requires codes to identify the nature of the injury, the affected body part, and the cause of the injury. Accurate and complete information is vital for processing the claim efficiently.
What should an employer do after submitting the Alabama First Report form?
After submitting the Alabama First Report form, the employer should ensure that they keep a copy for their records. It is also important to follow up with the insurance provider to confirm receipt of the form and to check on the status of the claim. Employers should maintain communication with the injured employee regarding their recovery and any necessary accommodations for their return to work. Additionally, employers should review their workplace safety practices to prevent future incidents and ensure compliance with Alabama's workers' compensation laws.
Incomplete Information: Failing to fill in all required fields can delay the processing of the report. Make sure to provide complete information for the employer, employee, and insurer sections.
Incorrect Codes: Using incorrect description codes for the nature of the injury, part of the body affected, and cause of injury can lead to misunderstandings. Always refer to the provided codes to ensure accuracy.
Missing Dates: Omitting critical dates, such as the date of injury or the date the employer was notified, can create complications. Ensure that all relevant dates are clearly stated.
Failure to Review: Not reviewing the completed form for errors before submission can result in mistakes going unnoticed. Take the time to double-check all entries for accuracy.
The Alabama First Report form is a critical document for employers to complete when an employee experiences a work-related injury or illness. However, there are several other forms and documents that often accompany this report to ensure compliance with state regulations and to facilitate the claims process. Below is a list of these important documents, each serving a specific purpose in the workers' compensation framework.
Understanding these forms and documents is crucial for both employers and employees navigating the workers' compensation process in Alabama. Each document plays a vital role in ensuring that claims are processed efficiently and that injured workers receive the benefits they are entitled to. Properly completing and submitting these forms can significantly impact the outcome of a claim, making it essential to approach this process with care and attention to detail.
The Alabama First Report form serves a crucial role in documenting workplace injuries and occupational diseases. Several other documents share similarities with this form in terms of purpose and content. Here are six such documents:
Understanding these documents can help employees and employers navigate the complexities of workplace injuries and ensure proper reporting and compliance.
When filling out the Alabama First Report form, attention to detail is crucial. Here are nine essential dos and don'ts to ensure your submission is accurate and timely.
By following these guidelines, you can help ensure that the Alabama First Report form is filled out correctly, minimizing delays and complications in the claims process.
Misconceptions about the Alabama First Report form can lead to confusion and errors in the reporting process. Here are seven common misconceptions clarified: