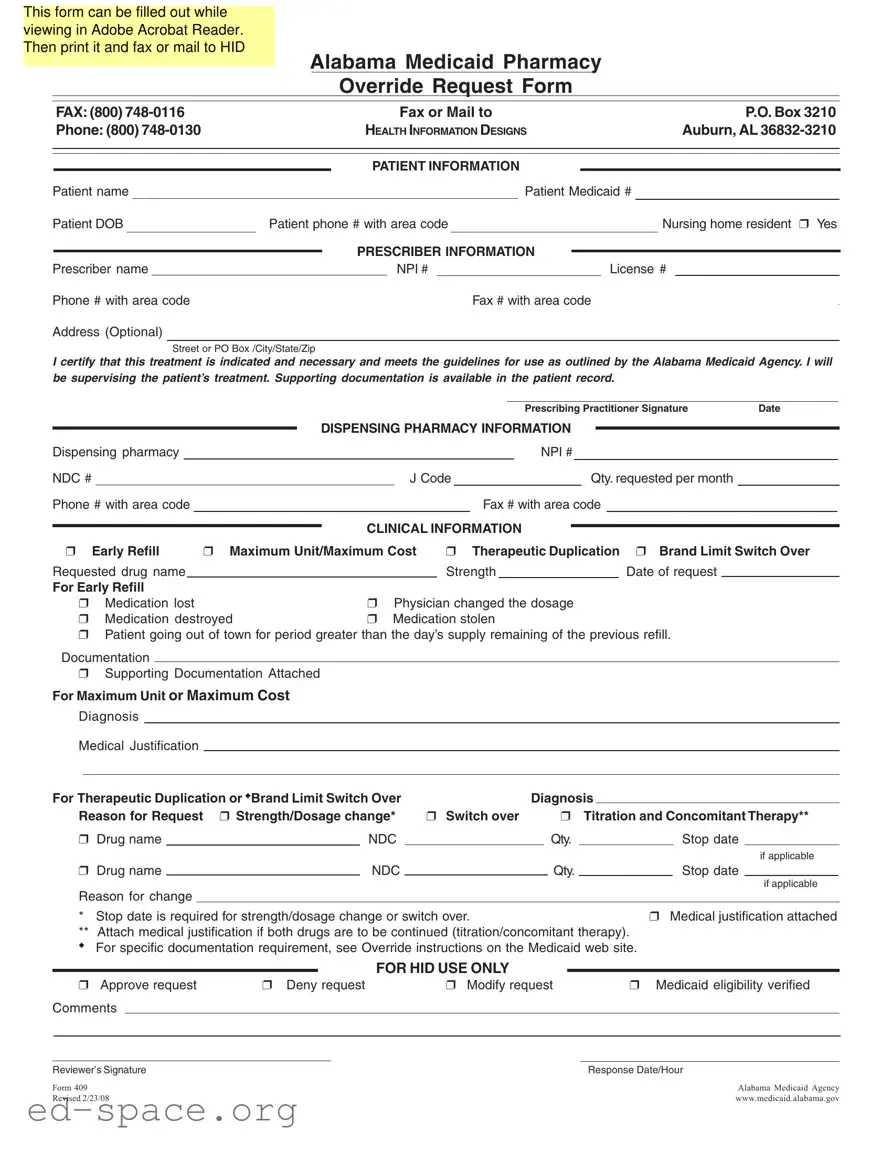
In Alabama, the 409 form serves a crucial role in the Medicaid system, streamlining the process for healthcare providers to request overrides for specific pharmacy needs. This form is designed to be user-friendly, allowing prescribers to fill it out easily while viewing it in Adobe Acrobat Reader. Once completed, it can be printed and submitted via fax or mail to the appropriate Medicaid office. Key sections of the form include patient information, prescriber details, and specific clinical justifications for the request. Providers must certify that the treatment is necessary and adheres to the guidelines set by the Alabama Medicaid Agency. Additionally, the form addresses various scenarios such as early refills, maximum unit requests, and therapeutic duplication, ensuring that all necessary information is captured for a comprehensive review. The form also allows for the inclusion of supporting documentation, which can be critical in justifying the request. Ultimately, the Alabama 409 form is an essential tool for ensuring that patients receive the medications they need in a timely manner, while also adhering to regulatory requirements.
This form can be filled out while viewing in Adobe Acrobat Reader. Then print it and fax or mail to HID
Alabama Medicaid Pharmacy
Override Request Form
FAX: (800) |
|
|
|
Fax or Mail to |
|
|
|
P.O. Box 3210 |
|
|||||||||||||
Phone: (800) |
|
|
HEALTH INFORMATION DESIGNS |
|
|
|
Auburn, AL |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient name |
|
|
|
|
|
|
|
|
Patient Medicaid # |
|
|
|||||||||||
Patient DOB |
Patient phone # with area code |
|
|
Nursing home resident ❒ Yes |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRESCRIBER INFORMATION |
|
|
|
|
|
|
|
|
|
|||||
Prescriber name |
|
|
|
|
|
License # |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
NPI # |
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Phone # with area code |
|
|
|
|
|
|
|
Fax # with area code |
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Address (Optional) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Street or PO Box /City/State/Zip
I certify that this treatment is indicated and necessary and meets the guidelines for use as outlined by the Alabama Medicaid Agency. I will be supervising the patient’s treatment. Supporting documentation is available in the patient record.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Prescribing Practitioner Signature |
Date |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
DISPENSING PHARMACY INFORMATION |
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Dispensing pharmacy |
|
|
|
|
|
|
|
|
NPI # |
|
|
|
|
|||||||||||
NDC # |
|
|
|
|
|
|
|
|
J Code |
|
|
|
|
|
|
Qty. requested per month |
|
|
||||||
Phone # with area code |
|
|
|
|
|
|
Fax # with area code |
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLINICAL INFORMATION |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
❒ |
Early Refill |
❒ Maximum Unit/Maximum Cost |
❒ |
Therapeutic Duplication |
❒ Brand Limit Switch Over |
|||||||||||||||||||
Requested drug name |
|
|
|
|
|
Strength |
|
|
Date of request |
|
|
|
||||||||||||
For Early Refill |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
❒ |
|
Medication lost |
|
|
❒ Physician changed the dosage |
|
|
|
|
|||||||||||||||
❒ |
|
Medication destroyed |
|
❒ Medication stolen |
|
|
|
|
||||||||||||||||
❒Patient going out of town for period greater than the day’s supply remaining of the previous refill.
Documentation
❒ Supporting Documentation Attached
For Maximum Unit or Maximum Cost
Diagnosis
Medical Justification
For Therapeutic Duplication or ◆Brand Limit Switch Over |
|
Diagnosis |
|
|||||||||
Reason for Request |
❒ Strength/Dosage change* |
❒ Switch over |
|
|
❒ |
Titration and Concomitant Therapy** |
||||||
❒ Drug name |
|
NDC |
|
|
|
Qty. |
|
|
Stop date |
|||
|
|
|
|
|
|
|
|
|
|
|
|
if applicable |
❒ Drug name |
|
NDC |
|
|
|
Qty. |
|
|
Stop date |
|||
|
|
|
|
|
|
|
|
|
|
|
|
if applicable |
Reason for change |
|
|
|
|
|
|
|
|
|
|
|
|
* Stop date is required for strength/dosage change or switch over. |
|
|
|
|
❒ Medical justification attached |
|||||||
**Attach medical justification if both drugs are to be continued (titration/concomitant therapy). ◆ For specific documentation requirement, see Override instructions on the Medicaid web site.
FOR HID USE ONLY
❒ Approve request |
❒ Deny request |
❒ Modify request |
❒ Medicaid eligibility verified |
||
Comments |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Reviewer’s Signature |
|
|
|
Response Date/Hour |
|
Form 409 |
|
|
|
Alabama Medicaid Agency |
|
Revised 2/23/08 |
|
|
|
www.medicaid.alabama.gov |
|
| Fact Name | Details |
|---|---|
| Purpose | The Alabama 409 form is used to request overrides for Medicaid pharmacy services, ensuring patients receive necessary medications. |
| Submission Method | This form can be filled out using Adobe Acrobat Reader, printed, and then faxed or mailed to the Alabama Medicaid Agency. |
| Contact Information | Requests can be faxed to (800) 748-0116 or mailed to P.O. Box 3210, Auburn, AL 36832-3210. |
| Patient Information Required | Essential details include the patient's name, Medicaid number, date of birth, and phone number. Indicating nursing home residency is also necessary. |
| Governing Law | The form is governed by Alabama Medicaid Agency guidelines, which outline the criteria for medication overrides. |
Filling out the Alabama 409 form is an important step in seeking approval for specific pharmacy requests. After completing the form, it can be printed and sent via fax or mail to the appropriate Medicaid office for processing.
What is the purpose of the Alabama 409 form?
The Alabama 409 form is used to request overrides for certain Medicaid pharmacy services. This form allows healthcare providers to obtain approval for early refills, maximum unit limits, therapeutic duplication, or brand limit switches. It ensures that the necessary treatments are indicated and meet the guidelines set by the Alabama Medicaid Agency.
How can I submit the Alabama 409 form?
You can fill out the Alabama 409 form using Adobe Acrobat Reader. After completing the form, print it and then submit it either by fax or mail. The fax number is (800) 748-0116, and you can mail it to P.O. Box 3210, Auburn, AL 36832-3210. For any questions, you can contact the Alabama Medicaid Pharmacy at (800) 748-0130.
What information is required on the Alabama 409 form?
The form requires detailed patient information, including the patient’s name, Medicaid number, date of birth, and phone number. Additionally, prescriber information such as the prescriber’s name, license number, and contact details must be provided. The dispensing pharmacy’s information, clinical details regarding the request, and supporting documentation are also necessary for processing.
What should I do if I need to provide supporting documentation?
If supporting documentation is required, ensure that it is attached to the Alabama 409 form before submission. This documentation may include medical justification for the request or any relevant patient records. For specific documentation requirements, refer to the override instructions available on the Alabama Medicaid website.
Missing Patient Information: Failing to provide complete patient details, such as the patient's name, Medicaid number, or date of birth, can delay the processing of the request.
Incorrect Prescriber Information: Not entering the prescriber's name, license number, or NPI number accurately can lead to confusion and rejection of the form.
Omitting Required Signatures: The prescribing practitioner’s signature is essential. Without it, the form is incomplete and cannot be processed.
Failure to Attach Supporting Documentation: When necessary, not including supporting documents can result in a denial of the request. Always check if additional information is needed.
Incorrectly Marking Clinical Information: Misidentifying the reason for the override request, such as selecting the wrong checkbox for early refill or therapeutic duplication, can lead to errors in processing.
Providing Incomplete Pharmacy Information: Missing details like the dispensing pharmacy’s NPI number or contact information can hinder communication and processing.
Not Following Up: After submitting the form, failing to check on the status can lead to missed opportunities for corrections or additional information requests.
Ignoring Submission Guidelines: Not faxing or mailing the form to the correct address or number can cause significant delays in the approval process.
The Alabama 409 form is a crucial document used for requesting overrides for Medicaid pharmacy services. However, several other forms and documents often accompany this request to ensure a comprehensive submission. Below is a list of these related documents, each serving a unique purpose in the Medicaid process.
Each of these documents plays a significant role in the Medicaid process, helping to streamline requests and ensure that patients receive the necessary care. Properly completing and submitting these forms can greatly impact the efficiency and success of the Medicaid pharmacy override request.
The Alabama 409 form is an important document used for requesting pharmacy overrides in the Medicaid system. Several other forms serve similar purposes in different contexts. Here are four documents that share similarities with the Alabama 409 form:
Each of these forms plays a critical role in ensuring that patients receive the medications they need while adhering to the guidelines set by healthcare providers and insurance companies.
When filling out the Alabama 409 form, attention to detail is crucial. Here are some important dos and don'ts to consider.
By following these guidelines, you can help ensure that your request is processed smoothly and efficiently.
Misconceptions about the Alabama 409 form can lead to confusion and errors in the submission process. Here are five common misconceptions:
When filling out and using the Alabama 409 form, consider the following key takeaways:
Following these guidelines will help ensure that the form is completed correctly and submitted effectively.