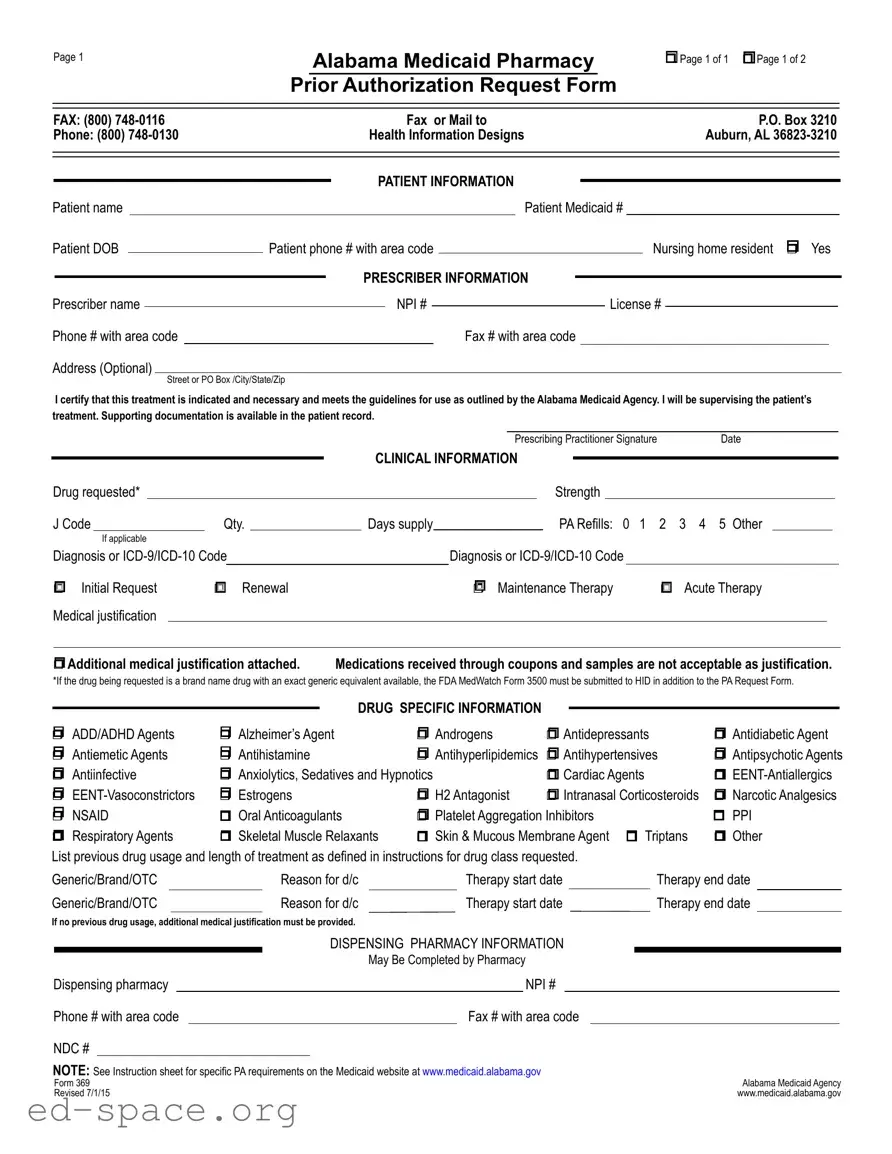
The Alabama 369 form serves as a crucial tool for healthcare providers seeking prior authorization for medications under the Alabama Medicaid program. This form is designed to streamline the process of obtaining necessary approvals for various pharmaceutical treatments, ensuring that patients receive the medications they need while adhering to state guidelines. It includes essential sections for patient information, prescriber details, and clinical specifics, allowing for a comprehensive overview of the request. The form prompts providers to specify the drug requested, its strength, and the relevant diagnosis codes, while also requiring medical justification for the prescribed therapy. Additionally, it addresses various drug categories, from antidepressants to antipsychotics, ensuring that all relevant information is captured for the review process. Providers are also encouraged to include any supporting documentation that may bolster the request, particularly in cases of previous drug usage or complex treatment plans. By providing a structured approach to medication requests, the Alabama 369 form plays a vital role in facilitating access to necessary treatments for Medicaid recipients.

Page 1
Alabama Medicaid Pharmacy
Prior Authorization Request Form
rPage 1 of 1 r Page 1 of 2
FAX: (800) |
|
|
|
Fax or Mail to |
|
|
|
|
P.O. Box 3210 |
|
|||||||||||||
Phone: (800) |
|
|
Health Information Designs |
|
|
|
|
Auburn, AL |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Patient name |
|
|
|
|
|
|
|
|
Patient Medicaid # |
|
|
||||||||||||
Patient DOB |
|
|
Patient phone # with area code |
|
|
|
|
Nursing home resident r Yes |
|
||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
PRESCRIBER INFORMATION |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Prescriber name |
|
|
|
|
|
|
NPI # |
|
|
|
|
License # |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Phone # with area code |
|
|
|
|
|
|
Fax # with area code |
|
|
|
|
|
|
|
|
||||||||
Address (Optional) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
I certify that this treatment is indicated and necessary and meets the guidelines for use as outlined by the Alabama Medicaid Agency. I will be supervising the patient’s treatment. Supporting documentation is available in the patient record.
|
|
|
|
|
|
|
|
|
|
|
|
|
Prescribing Practitioner Signature |
Date |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLINICAL INFORMATION |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Drug requested* |
|
|
|
|
|
|
|
|
|
|
|
Strength |
|
|
|
|
|
|
|
||||
|
J Code |
Qty. |
|
Days supply |
|
|
|
PA Refills: 0 1 |
2 3 4 5 Other |
|
||||||||||||||
|
|
If applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Diagnosis or |
|
|
|
Diagnosis or |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
r Initial Request |
r Renewal |
|
|
|
r |
Maintenance Therapy |
r Acute Therapy |
|
|||||||||||||||
|
Medical justification |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
r Additional medical justification attached. |
Medications received through coupons and samples are not acceptable as justification. |
|
|||||||||||||||||||||
*If the drug being requested is a brand name drug with an exact generic equivalent available, the FDA MedWatch Form 3500 must be submitted to HID in addition to the PA Request Form.
|
|
|
|
|
|
|
|
|
|
DRUG SPECIFIC INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
||
r ADD/ADHD Agents |
r Alzheimer’s Agent |
r Androgens |
r Antidepressants |
r Antidiabetic Agent |
|||
r Antiemetic Agents |
r Antihistamine |
r Antihyperlipidemics |
r Antihypertensives |
r Antipsychotic Agents |
|||
r Antiinfective |
r Anxiolytics, Sedatives and Hypnotics |
r Cardiac Agents |
r |
||||
r |
r Estrogens |
r H2 Antagonist |
r Intranasal Corticosteroids |
r Narcotic Analgesics |
|||
r NSAID |
r Oral Anticoagulants |
r Platelet Aggregation Inhibitors |
r PPI |
||||
r Respiratory Agents |
r Skeletal Muscle Relaxants |
r Skin & Mucous Membrane Agent r Triptans |
r Other |
||||
List previous drug usage and length of treatment as defined in instructions for drug class requested. |
|
|
|
|
||||||||||||||
Generic/Brand/OTC |
|
Reason for d/c |
|
Therapy start date |
|
|
Therapy end date |
|
||||||||||
Generic/Brand/OTC |
|
Reason for d/c |
|
Therapy start date |
|
Therapy end date |
|
|||||||||||
If no previous drug usage, additional medical justification must be provided. |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISPENSING PHARMACY INFORMATION |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
May Be Completed by Pharmacy |
|
|
|
|
|||||
Dispensing pharmacy |
|
|
|
|
|
NPI # |
|
|
|
|
|
|||||||
Phone # with area code |
|
|
|
|
Fax # with area code |
|
|
|
|
|
||||||||
NDC # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
NOTE: See Instruction sheet for specific PA requirements on the Medicaid website at www.medicaid.alabama.gov |
|
Alabama Medicaid Agency |
||||||||||||||||
Form 369 |
|
|
|
|
|
|
|
|
|
|||||||||
Revised 7/1/15 |
|
|
|
|
|
|
|
|
|
www.medicaid.alabama.gov |
||||||||
Page 2 |
Patient Medicaid # |
rSustained Release Oral Opioid Agonist
Proposed duration of therapy |
|
|
|
|
Is medicine for PRN use? |
r Yes |
r No |
|
|||
Type of pain r Acute r Chronic |
|
|
|
Severity of pain: r Mild |
r Moderate r Severe |
|
|||||
Is there a history of substance abuse or addiction? r Yes |
r No |
|
|
|
|||||||
If yes, is treatment plan attached? |
r Yes r No |
|
|
|
|
|
|
|
|
||
Indicate prior and/or current analgesic therapy and alternative management choices |
|
|
|
||||||||
Drug/therapy |
|
|
|
|
Reason for d/c |
|
|
|
|
|
|
Drug/therapy |
|
|
|
Reason for d/c |
|
|
|
|
|||
|
|
|
|
|
|||||||
r Antipsychotic Agents |
The request is for: |
r Monotherapy or r Polytherapy |
|
|
|||||||
For children < 6 years of age, have monitoring protocols (see Attachment C on the Alabama Medicaid website) been followed? r Yes r No For polytherapy and/or
Medical justification may include peer reviewed literature, medical record documentation, chart notes with specific symptoms that the support the diagnosis, etc.
rXenicalR
r |
If initial request |
Weight |
|
kg. |
|
Height |
|
inches |
BMI |
|
|
kg/m2 |
|||
r |
If renewal request |
Previous weight |
|
|
|
kg. |
Current weight |
|
|
|
kg. |
|
|
||
Documentation MD supervised exercise/diet regimen > 6 mo.? r Yes |
r No |
Planned adjunctive therapy? r Yes |
r No |
||||||||||||
r Phosphodiesterase Inhibitors |
|
|
|
|
|
|
|
|
||
Failure or inadequate response to the following alternate therapies: |
|
|
|
|
|
|||||
1. |
|
|
|
2. |
|
|
3. |
|
|
|
4. |
|
|
|
5. |
|
|
6. |
|
|
|
Contraindication of alternate therapies: |
|
|
|
|
|
|
|
|
||
r Documentation of vasoreactivity test attached |
r Consultation with specialist attached |
|
|
|||||||
|
|
|
|
|
|
|||||
r Specialized Nutritionals |
Height |
inches |
Current weight |
kg. |
|
|||||
rIf < 21 years of age, record supports that > 50% of need is met by specialized nutrition
rIf > 21 years of age, record supports 100% of need is met by specialized nutrition
Method of administration |
|
Duration |
|
|
|
|
# of refills |
|||
|
|
|
|
|
|
|
|
|
|
|
r Xolair® |
Current Weight:__________kg (patient’s weight must be between |
|||||||||
Is the patient 12 years or older? |
|
|
|
r |
Yes |
r |
No |
|||
Is the request for chronic idiopathic urticaria? |
r |
Yes |
r |
No |
||||||
Is the request for moderate to severe asthma and is treatment recommended by a board |
|
|
|
|
|
|
|
|||
certified pulmonologist or allergist after their evaluation (if yes answers questions below)? |
r |
Yes |
r |
No |
||||||
Has the patient had a positive skin or blood test reaction to a perennial aeroallergen? |
r |
Yes |
r |
No |
||||||
Is the patient symptomatic despite receiving a combination of either inhaled corticosteroid |
|
|
|
|
|
|
|
|||
and a leukotriene inhibitor or an inhaled corticosteroid and long acting beta agonist or has |
|
|
|
|
|
|
|
|||
the patient required 3 or more bursts of oral steroids within the past 12 months? |
r |
Yes |
r |
No |
||||||
Are the patient’s baseline IgE levels between 30 IU/mL and 700 IU/mL? |
r |
Yes |
r |
No |
||||||
Level:_________________ |
Date:__________________ |
|
|
|
|
|
|
|
||
Form 369 |
Alabama Medicaid Agency |
Revised |
www.medicaid.alabama.gov |
| Fact Name | Details |
|---|---|
| Purpose | The Alabama 369 form is used to request prior authorization for Medicaid pharmacy services, ensuring that prescribed medications meet the necessary guidelines. |
| Governing Law | This form is governed by the regulations set forth by the Alabama Medicaid Agency, specifically under the Alabama Medicaid Administrative Code. |
| Patient Information | It requires detailed patient information, including the patient’s name, Medicaid number, date of birth, and contact information. |
| Prescriber Certification | Prescribers must certify that the requested treatment is necessary and that they will supervise the patient’s treatment, ensuring accountability. |
| Documentation Requirements | Supporting documentation must be provided to justify the request, particularly for specific drug classes or if prior therapies have been ineffective. |
Filling out the Alabama 369 form requires careful attention to detail. Ensure that all necessary information is provided accurately to facilitate the processing of the request. Follow the steps outlined below to complete the form correctly.
Once the form is filled out, it can be faxed or mailed to the provided address. Ensure that all required documentation is attached to avoid delays in processing the request.
What is the Alabama 369 form used for?
The Alabama 369 form is primarily utilized for requesting prior authorization for pharmacy services under the Alabama Medicaid program. This form is essential for healthcare providers to obtain approval for specific medications that may not be automatically covered by Medicaid. By submitting this form, prescribers can demonstrate that a particular treatment is medically necessary and adheres to the guidelines set forth by the Alabama Medicaid Agency.
Who needs to fill out the Alabama 369 form?
The form must be completed by the prescriber, who is responsible for the patient's treatment. This includes physicians, nurse practitioners, and physician assistants. It requires detailed patient information, including the patient's Medicaid number, date of birth, and contact details. Additionally, the prescriber must provide their own information, including their name, National Provider Identifier (NPI), and license number.
What information is required on the Alabama 369 form?
Several key pieces of information are needed on the Alabama 369 form. This includes the patient's demographics, the medication requested, its strength, quantity, and the diagnosis codes. The prescriber must also indicate whether the request is for an initial request, renewal, or maintenance therapy. Medical justification for the requested medication must be provided, along with any previous drug usage history if applicable. Supporting documentation may also be required to substantiate the request.
How is the Alabama 369 form submitted?
The completed Alabama 369 form can be submitted via fax or mail. The fax number for submissions is (800) 748-0116, and it can also be mailed to Health Information Designs at P.O. Box 3210, Auburn, AL 36823-3210. It’s crucial to ensure that all required information is accurately filled out to avoid delays in processing the authorization request.
What happens after the Alabama 369 form is submitted?
Once the form is submitted, the Alabama Medicaid Agency will review the request to determine if the medication meets the necessary criteria for coverage. The prescriber will receive notification regarding the approval or denial of the request. If approved, the patient can proceed to obtain the medication. If denied, the prescriber may need to provide additional information or consider alternative treatments.
Incomplete Patient Information: Failing to provide all necessary patient details, such as the patient's name, Medicaid number, or date of birth, can lead to delays in processing the request.
Missing Prescriber Information: Omitting crucial information about the prescriber, including their name, NPI number, or contact details, may result in the form being rejected.
Insufficient Clinical Justification: Not providing adequate medical justification for the requested drug can hinder approval. Supporting documentation must be attached when necessary.
Incorrect Drug Information: Entering incorrect drug names, strengths, or quantities can cause confusion and may lead to denial of the request.
Failure to Indicate Previous Drug Usage: Not listing previous medications and their usage can result in the need for additional justification, slowing down the process.
Neglecting to Check Required Boxes: Failing to mark essential checkboxes, such as whether the request is for an initial request or a renewal, can lead to processing errors.
Not Following Submission Guidelines: Not adhering to the specific submission requirements outlined by the Alabama Medicaid Agency, such as faxing or mailing to the correct address, may result in delays or rejections.
The Alabama 369 form is an essential document used for requesting prior authorization for Medicaid pharmacy services in Alabama. Along with this form, several other documents may be necessary to support the request and ensure compliance with Medicaid guidelines. Below is a list of commonly used forms and documents that often accompany the Alabama 369 form.
These documents collectively help facilitate the prior authorization process, ensuring that patients receive the medications they need while complying with Medicaid regulations. Having all necessary forms ready can significantly streamline the approval process and improve patient care outcomes.
The Alabama 369 form is a specific document used for requesting prior authorization for medications under Alabama Medicaid. Several other forms serve similar purposes in different contexts or jurisdictions. Here are nine documents that are comparable to the Alabama 369 form:
Each of these documents serves to ensure that the requested treatments or medications are necessary and appropriate, reflecting the goal of the Alabama 369 form in the context of Medicaid. They require similar information regarding patient details, prescriber information, and medical justification.
When filling out the Alabama 369 form, it is important to follow specific guidelines to ensure accuracy and compliance. Below are seven key points to consider, including actions to take and avoid.
By adhering to these guidelines, the likelihood of a smooth approval process increases significantly. Proper attention to detail is essential for both patients and providers.
Understanding the Alabama 369 form can be challenging, and several misconceptions can lead to confusion. Here’s a list of common misunderstandings, along with clarifications to help you navigate the process more effectively.
By addressing these misconceptions, patients and providers can better understand the Alabama 369 form and navigate the prior authorization process more effectively.
When filling out the Alabama 369 form, there are several key points to keep in mind to ensure a smooth process for your Medicaid Pharmacy Prior Authorization request. Here are some essential takeaways:
Filling out the Alabama 369 form accurately is essential for ensuring that patients receive the medications they need in a timely manner. By following these guidelines, you can help facilitate the authorization process effectively.