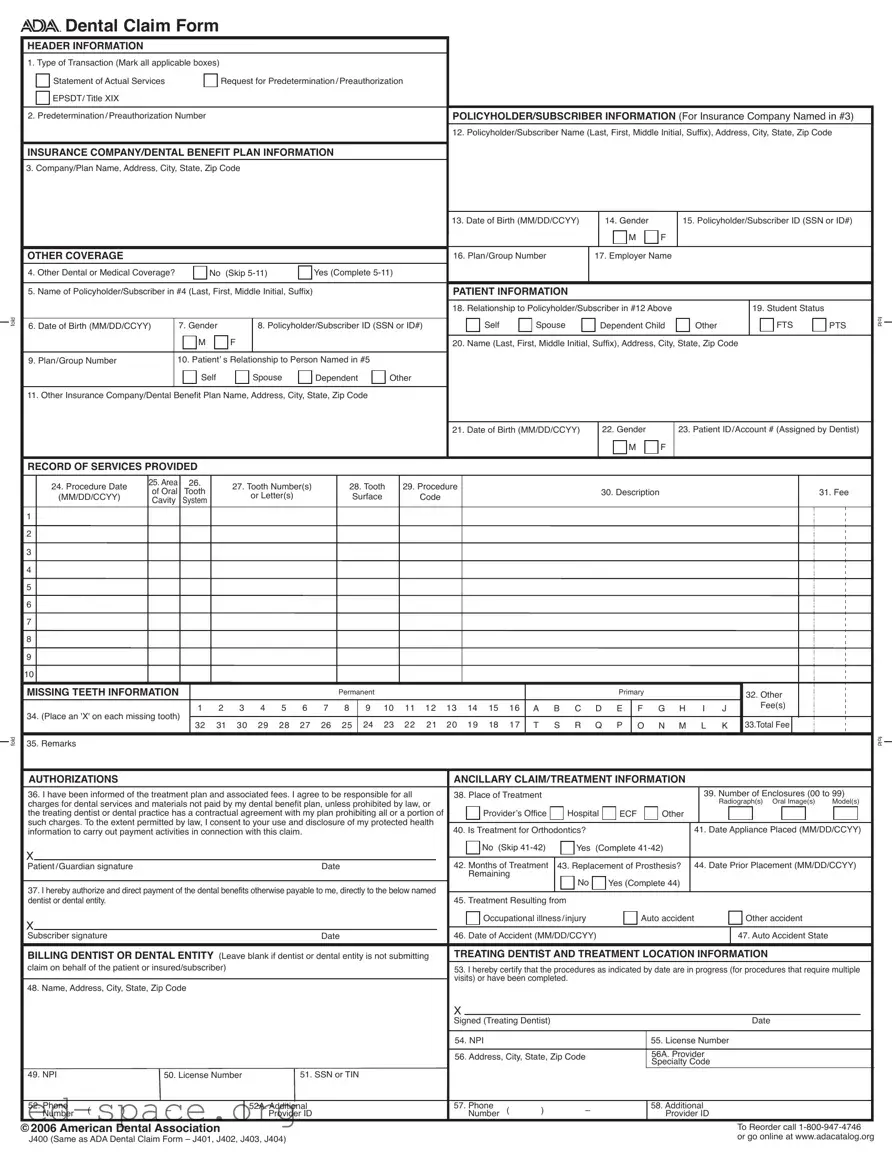
The ADA Dental Claim Form serves as a crucial document in the process of seeking reimbursement for dental services. It is structured to collect essential information about the transaction, policyholder, patient, and services provided. The header section requires the type of transaction, such as a statement of actual services or a request for predetermination, ensuring clarity in the claim's purpose. Details about the policyholder, including name, address, and subscriber ID, must be accurately filled out to facilitate communication with the insurance company. The form also addresses any other dental or medical coverage that the patient may have, which is vital for coordinating benefits. Patient information, including their relationship to the policyholder and relevant demographic details, is collected to establish eligibility for coverage. Furthermore, the record of services provided section outlines specific procedures performed, associated fees, and missing teeth information, if applicable. This comprehensive format ensures that all necessary data is presented clearly and concisely, aiding in the timely processing of claims. The form also includes authorizations for treatment and payment, as well as sections for the treating dentist’s information, thus streamlining the claim submission process while maintaining compliance with regulations.
fold
fold
Dental Claim Form
HEADER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. Type of Transaction (Mark all applicable boxes) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Statement of Actual Services |
|
|
Request for Predetermination/Preauthorization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
EPSDT/ Title XIX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Predetermination/Preauthorization Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POLICYHOLDER/SUBSCRIBER INFORMATION (For Insurance Company Named in #3) |
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. Policyholder/Subscriber Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
INSURANCE COMPANY/DENTAL BENEFIT PLAN INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
3. Company/Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. Date of Birth (MM/DD/CCYY) |
|
|
14. Gender |
|
|
15. Policyholder/Subscriber ID (SSN or ID#) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
OTHER COVERAGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16. Plan/Group Number |
|
|
17. Employer Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
4. Other Dental or Medical Coverage? |
|
|
No (Skip |
|
|
Yes (Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
5. Name of Policyholder/Subscriber in #4 (Last, First, Middle Initial, Suffix) |
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. Relationship to Policyholder/Subscriber in #12 Above |
|
|
|
|
|
|
|
19. Student Status |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Self |
|
Spouse |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FTS |
PTS |
fold |
|||||||||
6. Date of Birth (MM/DD/CCYY) |
|
7. Gender |
|
|
|
8. Policyholder/Subscriber ID (SSN or ID#) |
|
|
|
Dependent Child |
Other |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
M |
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
9. Plan/Group Number |
|
|
10. Patient’ s Relationship to Person Named in #5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
Self |
|
|
|
Spouse |
|
Dependent |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
11. Other Insurance Company/Dental Benefit Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. Date of Birth (MM/DD/CCYY) |
|
|
22. Gender |
|
|
23. Patient ID/Account # (Assigned by Dentist) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
RECORD OF SERVICES PROVIDED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24. Procedure Date |
25. Area |
26. |
|
27. Tooth Number(s) |
|
|
28. Tooth |
29. Procedure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
of Oral |
Tooth |
|
|
|
|
|
|
|
|
|
30. Description |
|
|
|
|
|
|
|
|
|
|
|
31. Fee |
|
||||||||||||||||||||||||||||
|
(MM/DD/CCYY) |
|
|
|
|
or Letter(s) |
|
|
|
Surface |
Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
Cavity |
System |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
MISSING TEETH INFORMATION |
|
|
|
|
|
|
|
|
|
|
Permanent |
|
|
|
|
|
|
|
|
|
|
Primary |
|
|
|
|
|
|
|
|
|
32. Other |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
8 |
|
9 10 11 12 13 14 15 16 |
A B C D E |
F G H |
|
I |
J |
|
|
|
|
Fee(s) |
|
|
|
|
|
|
|
|||||||||||||||||||
34. (Place an 'X' on each missing tooth) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
32 |
31 |
30 |
29 |
28 |
27 |
26 |
|
25 |
|
24 23 |
22 21 |
|
20 19 18 |
17 |
T |
S R |
Q |
P |
O |
N M |
|
L |
K 33.Total Fee |
|
|
|
|
|
|
|
||||||||||||||||
35. Remarks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
fold |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
AUTHORIZATIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ANCILLARY CLAIM/TREATMENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
36. I have been informed of the treatment plan and associated fees. I agree to be responsible for all |
38. Place of Treatment |
|
|
|
|
|
|
|
|
|
|
|
|
39. Number of Enclosures (00 to 99) |
|
||||||||||||||||||||||||||||||||||||||
charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Radiograph(s) Oral Image(s) |
Model(s) |
|
|||||||||||||||||||||||||||||||||
the treating dentist or dental practice has a contractual agreement with my plan prohibiting all or a portion of |
|
Provider’s Office |
Hospital |
ECF |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
such charges. To the extent permitted by law, I consent to your use and disclosure of my protected health |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
information to carry out payment activities in connection with this claim. |
|
|
|
|
|
|
|
40. Is Treatment for Orthodontics? |
|
|
|
|
|
|
|
|
|
41. Date Appliance Placed (MM/DD/CCYY) |
|
||||||||||||||||||||||||||||||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No (Skip |
Yes |
(Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient/Guardian signature |
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
42. Months of Treatment |
43. Replacement of Prosthesis? |
|
44. Date Prior Placement (MM/DD/CCYY) |
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
37. I hereby authorize and direct payment of the dental benefits otherwise payable to me, directly to the below named |
|
|
|
|
No |
|
|
Yes (Complete 44) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
dentist or dental entity. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
45. Treatment Resulting from |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupational illness/injury |
|
|
|
Auto accident |
|
|
|
|
|
Other accident |
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Subscriber signature |
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
46. Date of Accident (MM/DD/CCYY) |
|
|
|
|
|
|
|
|
|
|
47. Auto Accident State |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
BILLING DENTIST OR DENTAL ENTITY (Leave blank if dentist or dental entity is not submitting |
TREATING DENTIST AND TREATMENT LOCATION INFORMATION |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
claim on behalf of the patient or insured/subscriber) |
|
|
|
|
|
|
|
|
|
|
|
|
|
53. I hereby certify that the procedures as indicated by date are in progress (for procedures that require multiple |
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
visits) or have been completed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
48. Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signed (Treating Dentist) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
54. NPI |
|
|
|
|
|
|
|
|
|
55. License Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
56. Address, City, State, Zip Code |
|
|
|
|
|
56A. Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Specialty Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
49. NPI |
|
|
50. License Number |
|
|
|
51. SSN or TIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
52. Phone |
( |
) |
– |
|
|
|
|
|
52A. Additional |
|
|
|
|
|
|
|
57. Phone |
( |
) |
– |
|
|
|
|
|
58. Additional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Number |
|
|
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
Number |
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
©2006 American Dental Association |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To Reorder call |
|
||||||||||||||||||||
J400 (Same as ADA Dental Claim Form – J401, J402, J403, J404) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or go online at www.adacatalog.org |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
| Fact Name | Details |
|---|---|
| Type of Transaction | The form allows for multiple types of transactions, including a Statement of Actual Services, Request for Predetermination/Preauthorization, and EPSDT/Title XIX. |
| Policyholder Information | It requires the Policyholder/Subscriber's full name, address, and date of birth. |
| Insurance Company Details | The form must include the name and address of the insurance company or dental benefit plan. |
| Other Coverage | If there is other dental or medical coverage, additional information must be provided, including the name of the policyholder. |
| Patient Information | Details about the patient, including their relationship to the policyholder, must be filled out accurately. |
| Record of Services Provided | Providers must document the procedure date, area, tooth number, and fees for services rendered. |
| Authorization Section | The patient or guardian must sign to authorize payment of benefits directly to the dentist or dental entity. |
| Coordination of Benefits | When submitting to a secondary payer, the primary payer's Explanation of Benefits (EOB) must be attached. |
| State-Specific Regulations | Each state may have specific laws governing the use of the ADA Dental Claim Form, which should be reviewed for compliance. |
Completing the ADA Dental Claim Form requires careful attention to detail to ensure all necessary information is provided accurately. Following these steps will help streamline the process and facilitate timely processing of the claim.
After filling out the form, review it for accuracy. Ensure that all necessary signatures are obtained. Once everything is complete, submit the form to the insurance company or dental benefit plan as instructed. This will initiate the claims process, allowing for the review and potential reimbursement for the dental services provided.
What is the ADA Dental Claim Form used for?
The ADA Dental Claim Form is a standardized document used to submit claims for dental services to insurance companies or dental benefit plans. It helps ensure that all necessary information is provided for the processing of claims, facilitating reimbursement for dental care received by patients.
What information is required in the header section of the form?
The header section requires details about the type of transaction, such as whether it is a statement of actual services or a request for preauthorization. Additionally, it includes a space for the predetermination or preauthorization number, if applicable.
How should I fill out the policyholder/subscriber information?
This section must include the policyholder's or subscriber's full name, address, and date of birth. The gender and identification number, either Social Security Number or another ID, must also be provided. Accurate completion of this section ensures that the claim is linked to the correct insurance policy.
What should I do if the patient has other dental or medical coverage?
If the patient has additional coverage, you must complete the sections related to other coverage. This includes providing the name of the policyholder for the other insurance and the relevant details about that plan. If there is no other coverage, simply skip to the patient information section.
How do I document the services provided on the form?
In the Record of Services Provided section, you must enter the procedure date, area, tooth numbers, and a description of the services rendered. Each procedure should be listed clearly, and the associated fees must be documented accurately to facilitate payment processing.
What if the number of procedures exceeds the available lines on the form?
If you have more procedures than can fit on one claim form, you should list the remaining procedures on a separate, fully completed claim form. Each claim should be submitted with the necessary details to avoid delays in processing.
What is the purpose of the authorization section?
The authorization section allows the patient or guardian to acknowledge their understanding of the treatment plan and associated fees. By signing this section, they agree to be responsible for any charges not covered by their dental benefit plan, ensuring transparency in financial responsibilities.
How is the National Provider Identifier (NPI) used on the form?
The NPI is a unique identifier assigned to healthcare providers, including dentists. It must be included in the appropriate sections of the claim form to ensure that the services are correctly attributed to the provider. This identifier is essential for compliance with HIPAA regulations.
What should I do if the treatment is related to an accident?
If the dental treatment results from an accident, you must indicate this in the designated section of the form. You will also need to provide details about the accident, including the date and nature of the incident, which may affect the claim's processing.
Where can I find more information about completing the ADA Dental Claim Form?
Comprehensive instructions for completing the ADA Dental Claim Form can be found in Section 4 of the ADA Publication titled CDT-2007/2008. Updates and additional resources are also available on the ADA's official website, ensuring that you have the most current information for accurate claim submission.
Failing to mark all applicable transaction types in the header section. It's important to indicate if you're submitting a statement of services, a request for predetermination, or other relevant options.
Not including the predetermination or preauthorization number if applicable. This number is crucial for processing your claim efficiently.
Leaving out the policyholder's name and full address. Ensure you provide the complete details as this is essential for the insurance company to process the claim.
Omitting the patient's relationship to the policyholder. This information helps clarify the connection between the patient and the insurance holder.
Not providing the patient's date of birth in the correct format (MM/DD/CCYY). Incorrect date formats can lead to processing delays.
Failing to fill out the record of services provided section completely. Each procedure must be documented accurately, including dates and fees.
Forgetting to sign the authorization section. Without your signature, the claim cannot be processed.
Neglecting to attach the primary payer's Explanation of Benefits (EOB) when submitting to a secondary payer. This is essential for coordination of benefits.
Not indicating missing teeth properly. Use the designated area to mark any missing teeth, as this can affect the claim outcome.
Leaving out the National Provider Identifier (NPI) for the dentist. This identifier is necessary for identification and billing purposes.
When submitting a dental claim, several additional forms and documents may be required to ensure a smooth processing experience. Each document serves a specific purpose and helps provide necessary information to the insurance company or dental benefit plan.
Using these documents in conjunction with the ADA Dental Claim Form can streamline the claims process and help avoid delays. Ensure all forms are completed accurately to facilitate timely reimbursement.
When filling out the ADA Dental Claim Form, consider the following guidelines to ensure a smooth submission process.
This form is versatile. It can also be used for preauthorization requests and other types of dental claims. Understanding its full range of applications can help streamline the claims process.
While it is essential to provide complete information, not all fields are mandatory for every situation. Some sections can be skipped based on specific circumstances, such as when there is no other coverage.
When submitting a claim to a secondary payer, attaching the primary payer's EOB is crucial. This document outlines what was paid by the first insurer and helps in processing the claim accurately.
While some dentists may choose to obtain an NPI, it is mandatory for those considered HIPAA covered entities. This identifier is essential for processing claims and ensuring compliance with federal regulations.
Providing details about missing teeth is often required. This information can impact the treatment plan and reimbursement process, making it vital to include on the claim form.
Ensure all required fields are filled out completely. Missing information can delay processing.
Use the correct transaction type. Indicate whether you are submitting a statement of services, a request for preauthorization, or other options.
Provide accurate policyholder information. Include the full name, address, and subscriber ID.
When indicating other coverage, complete the relevant sections only if applicable.
Document patient information thoroughly, including relationship to the policyholder and date of birth.
List all services provided with precise dates and codes. This ensures clarity for the insurance provider.
Include the total fee for services rendered. Double-check calculations for accuracy.
Sign and date the authorization section. This confirms your agreement to the treatment plan and payment responsibilities.
Attach any necessary documents, such as the primary payer's Explanation of Benefits, when submitting to a secondary payer.